

Cost-Effectiveness of Left Atrial Appendage Closure for Stroke Reduction in Atrial Fibrillation: Analysis of Pooled, 5-Year, Long-Term Data
- PMID: 31230500
- PMCID: PMC6662368
- DOI: 10.1161/JAHA.118.011577
Cost-Effectiveness of Left Atrial Appendage Closure for Stroke Reduction in Atrial Fibrillation: Analysis of Pooled, 5-Year, Long-Term Data
Abstract
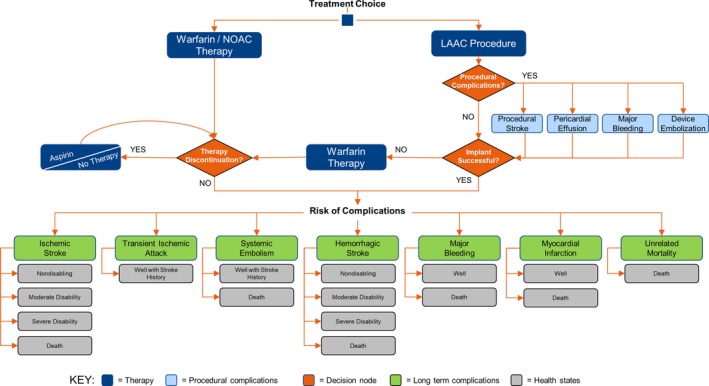
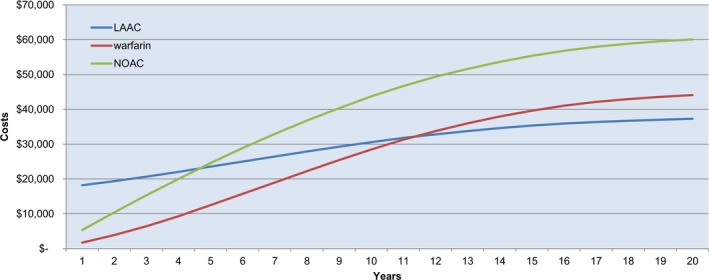
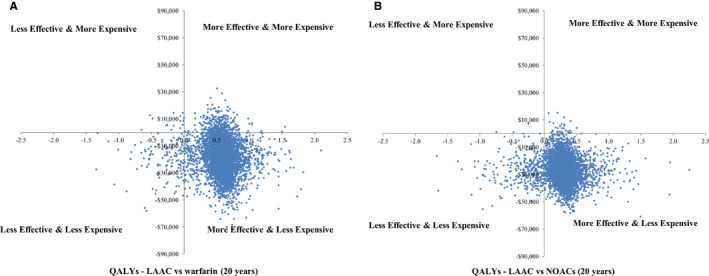
Background Recent publications reached conflicting conclusions about the cost-effectiveness of left atrial appendage closure (LAAC) with the Watchman device (Boston Scientific, Marlborough, MA) for stroke risk reduction in nonvalvular atrial fibrillation (AF). This analysis sought to assess the cost-effectiveness of LAAC relative to both warfarin and nonwarfarin oral anticoagulants (NOACs) using pooled, long-term data from the randomized PROTECT AF (Watchman Left Atrial Appendage System for Embolic Protection in Patients With Atrial Fibrillation) and PREVAIL (Prospective Randomized Evaluation of the Watchman LAA Closure Device in Patients With Atrial Fibrillation Versus Long-Term Warfarin) trials. Methods and Results A Markov model was constructed from a US payer perspective with a lifetime (20-year) horizon. LAAC clinical event rates and stroke outcomes were from pooled PROTECT AF and PREVAIL trial 5-year data. Warfarin and NOAC inputs were derived from published meta-analyses. The model was populated with a cohort of 10 000 patients, aged 70 years, at moderate stroke and bleeding risk. Sensitivity analyses were performed. LAAC was cost-effective relative to warfarin by year 7 ($48 674/quality-adjusted life-year) and dominant (more effective and less costly) by year 10. LAAC became cost-effective and dominant compared with NOACs by year 5. Over a lifetime, LAAC provided 0.60 more quality-adjusted life-years than warfarin and 0.29 more than NOACs. In sensitivity analyses, LAAC was cost-effective relative to warfarin and NOACs in 98% and 95% of simulations, respectively. Conclusions Using pooled, 5-year PROTECT AF and PREVAIL trial data, LAAC proved to be not only cost-effective, but cost saving relative to warfarin and NOACs. LAAC with the Watchman device is an economically viable stroke risk reduction strategy for patients with AF seeking an alternative to lifelong anticoagulation.
Keywords: Watchman; anticoagulant; atrial fibrillation; cost‐effectiveness; left atrial appendage closure; nonwarfarin oral anticoagulants.
Figures
Similar articles
-
Time to Cost-Effectiveness Following Stroke Reduction Strategies in AF: Warfarin Versus NOACs Versus LAA Closure.J Am Coll Cardiol. 2015 Dec 22;66(24):2728-2739. doi: 10.1016/j.jacc.2015.09.084. Epub 2015 Nov 23. J Am Coll Cardiol. 2015. PMID: 26616031
-
Cost-effectiveness of left atrial appendage closure with Watchman for non-valvular atrial fibrillation patients in Japan.J Med Econ. 2023 Jan-Dec;26(1):1357-1367. doi: 10.1080/13696998.2023.2266275. Epub 2023 Oct 27. J Med Econ. 2023. PMID: 37819734
-
5-Year Outcomes After Left Atrial Appendage Closure: From the PREVAIL and PROTECT AF Trials.J Am Coll Cardiol. 2017 Dec 19;70(24):2964-2975. doi: 10.1016/j.jacc.2017.10.021. Epub 2017 Nov 4. J Am Coll Cardiol. 2017. PMID: 29103847 Clinical Trial.
-
Overview of the Food and Drug Administration circulatory system devices panel meetings on WATCHMAN left atrial appendage closure therapy.Am J Cardiol. 2015 Feb 1;115(3):378-84. doi: 10.1016/j.amjcard.2014.11.011. Epub 2014 Nov 12. Am J Cardiol. 2015. PMID: 25579887 Review.
-
Left Atrial Appendage Closure Device With Delivery System: A Health Technology Assessment.Ont Health Technol Assess Ser. 2017 Jul 4;17(9):1-106. eCollection 2017. Ont Health Technol Assess Ser. 2017. PMID: 28744335 Free PMC article.
Cited by
-
Cost-effectiveness analysis of left atrial appendage occlusion in patients with atrial fibrillation and contraindication to oral anticoagulation.Eur Heart J. 2022 Mar 31;43(13):1348-1356. doi: 10.1093/eurheartj/ehab847. Eur Heart J. 2022. PMID: 34919652 Free PMC article.
-
3-Year outcomes after left atrial appendage closure in patients with nonvalvular atrial fibrillation: cardiomyopathy related with increased death and stroke rate.BMC Cardiovasc Disord. 2023 Jan 17;23(1):27. doi: 10.1186/s12872-023-03054-9. BMC Cardiovasc Disord. 2023. PMID: 36650429 Free PMC article. Clinical Trial.
-
Improving Left Atrial Appendage Occlusion Device Size Determination by Three-Dimensional Printing-Based Preprocedural Simulation.Front Cardiovasc Med. 2022 Feb 16;9:830062. doi: 10.3389/fcvm.2022.830062. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35252401 Free PMC article.
-
2021 Focused update of the 2017 consensus guidelines of the Asia Pacific Heart Rhythm Society (APHRS) on stroke prevention in atrial fibrillation.J Arrhythm. 2021 Nov 13;37(6):1389-1426. doi: 10.1002/joa3.12652. eCollection 2021 Dec. J Arrhythm. 2021. PMID: 34887945 Free PMC article.
-
Cost-effectiveness of left atrial appendage closure for stroke prevention in atrial fibrillation: a systematic review appraising the methodological quality.Cost Eff Resour Alloc. 2023 Oct 23;21(1):76. doi: 10.1186/s12962-023-00486-0. Cost Eff Resour Alloc. 2023. PMID: 37872572 Free PMC article.
References
-
- Kim MH, Johnston SS, Chu BC, Dalal MR, Schulman KL. Estimation of total incremental health care costs in patients with atrial fibrillation in the United States. Circ Cardiovasc Qual Outcomes. 2011;4:313–320. - PubMed
-
- Kimmel SE, Chen Z, Price M, Parker CS, Metlay JP, Christie JD, Brensinger CM, Newcomb CW, Samaha FF, Gross R. The influence of patient adherence on anticoagulation control with warfarin results from the International Normalized Ratio adherence and genetics (IN‐RANGE) study. Arch Intern Med. 2007;167:229–235. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly PA, Themeles E, Varrone J, Wang S, Alings M, Xavier D, Zhu J, Diaz R, Lewis BS, Darius H, Diener HC, Joyner CD, Wallentin L; on behalf of RE‐LY Steering Committee and Investigators . Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–1151. - PubMed
-
- Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, Breithardt G, Halperin JL, Hankey GJ, Piccini JP, Becker RC, Nessel CC, Paolini JF, Berkowitz SD, Fox KA, Califf RM; on behalf of ROCKET AF Investigators. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883–891. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
