

Spironolactone in Acute Heart Failure Patients With Renal Dysfunction and Risk Factors for Diuretic Resistance: From the ATHENA-HF Trial
- PMID: 31230825
- PMCID: PMC6685766
- DOI: 10.1016/j.cjca.2019.01.022
Spironolactone in Acute Heart Failure Patients With Renal Dysfunction and Risk Factors for Diuretic Resistance: From the ATHENA-HF Trial
Abstract
Background: Acute heart failure (HF) patients with renal insufficiency and risk factors for diuretic resistance may be most likely to derive incremental improvement in congestion with the addition of spironolactone.
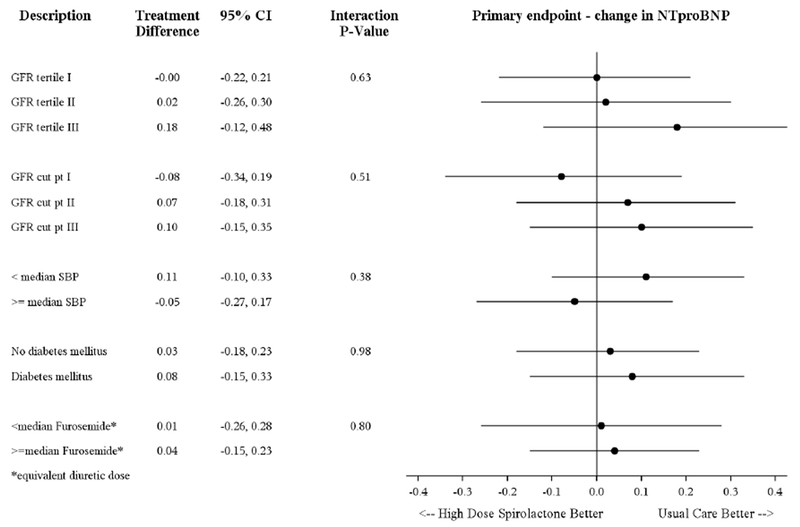
Methods: The Aldosterone Targeted Neurohormonal Combined with Natriuresis Therapy in Heart Failure (ATHENA-HF) trial randomized 360 acute HF patients with reduced or preserved ejection fraction to spironolactone 100 mg daily or usual care for 96 hours. The current analysis assessed the effects of study therapy within tertiles of baseline estimated glomerular filtration rate (eGFR) and subgroups at heightened risk for diuretic resistance.
Results: Across eGFR tertiles, there was no incremental benefit of high-dose spironolactone on any efficacy endpoint, including changes in log N-terminal pro-B-type natriuretic peptide and signs and symptoms of congestion (all P for interaction ≥ 0.06). High-dose spironolactone had no significant effect on N-terminal pro-B-type natriuretic peptide reduction regardless of blood pressure, diabetes mellitus status, and loop diuretic dose (all P for interaction ≥ 0.38). In-hospital changes in serum potassium and creatinine were similar between treatment groups for all GFR tertiles (all P for interaction ≥ 0.18). Rates of inpatient worsening HF, 30-day worsening HF, and 60-day all-cause mortality were numerically higher among patients with lower baseline eGFR, but relative effects of study treatment did not differ with renal function (all P for interaction ≥ 0.27).
Conclusions: High-dose spironolactone did not improve congestion over usual care among patients with acute HF, irrespective of renal function and risk factors for diuretic resistance. In-hospital initiation or continuation of spironolactone was safe during the inpatient stay, even when administered at high doses to patients with moderate renal dysfunction.
Trial registration: ClinicalTrials.gov NCT02235077.
Copyright © 2019 Canadian Cardiovascular Society. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Cardiorenal Interactions, Diuretic Resistance, and Acute Heart Failure: Renal Response vs Renal Function.Can J Cardiol. 2019 Sep;35(9):1079-1081. doi: 10.1016/j.cjca.2019.02.020. Epub 2019 Mar 1. Can J Cardiol. 2019. PMID: 31472805 No abstract available.
References
-
- Ambrosy AP, Pang PS, Khan S, Konstam MA, Fonarow GC, Traver B, Maggioni AP, Cook T, Swedberg K, Burnett JC Jr, Grinfeld L Udelson JE, Zannad F, Gheorghiade M and Investigators ET. Clinical course and predictive value of congestion during hospitalization in patients admitted for worsening signs and symptoms of heart failure with reduced ejection fraction: findings from the EVEREST trial. Eur Heart J. 2013;34:835–43. - PubMed
-
- Greene SJ, Fonarow GC, Vaduganathan M, Khan SS, Butler J and Gheorghiade M. The vulnerable phase after hospitalization for heart failure. Nat Rev Cardiol 2015;12:220–9. - PubMed
-
- Valente MA, Voors AA, Damman K, Van Veldhuisen DJ, Massie BM, O’Connor CM, Metra M, Ponikowski P, Teerlink JR, Cotter G, Davison B, Cleland JG, Givertz MM, Bloomfield DM, Fiuzat M, Dittrich HC and Hillege HL. Diuretic response in acute heart failure: clinical characteristics and prognostic significance. Eur Heart J. 2014;35:1284–93. - PubMed
-
- ter Maaten JM, Dunning AM, Valente MA, Damman K, Ezekowitz JA, Califf RM, Starling RC, van der Meer P, O’Connor CM, Schulte PJ, Testani JM, Hernandez AF, Tang WH and Voors AA. Diuretic response in acute heart failure-an analysis from ASCEND-HF. Am Heart J. 2015;170:313–21. - PubMed
-
- Voors AA, Davison BA, Teerlink JR, Felker GM, Cotter G, Filippatos G, Greenberg BH, Pang PS, Levin B, Hua TA, Severin T, Ponikowski P, Metra M and Investigators R-A. Diuretic response in patients with acute decompensated heart failure: characteristics and clinical outcome--an analysis from RELAX-AHF. Eur J Heart Fail 2014;16:1230–40. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1 TR002548/TR/NCATS NIH HHS/United States
- U10 HL110342/HL/NHLBI NIH HHS/United States
- T32 HL007101/HL/NHLBI NIH HHS/United States
- U10 HL084904/HL/NHLBI NIH HHS/United States
- U10 HL110312/HL/NHLBI NIH HHS/United States
- U10 HL110262/HL/NHLBI NIH HHS/United States
- T32 HL069749/HL/NHLBI NIH HHS/United States
- U10 HL110337/HL/NHLBI NIH HHS/United States
- T32 HL007604/HL/NHLBI NIH HHS/United States
- U10 HL110309/HL/NHLBI NIH HHS/United States
- U10 HL110336/HL/NHLBI NIH HHS/United States
- U10 HL110338/HL/NHLBI NIH HHS/United States
- U10 HL110302/HL/NHLBI NIH HHS/United States
- U10 HL110297/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
