

The missing piece: Clinical pharmacists enhancing the interprofessional nephrology clinic model
- PMID: 31231002
- PMCID: PMC8150925
- DOI: 10.1016/j.japh.2019.05.010
The missing piece: Clinical pharmacists enhancing the interprofessional nephrology clinic model
Abstract
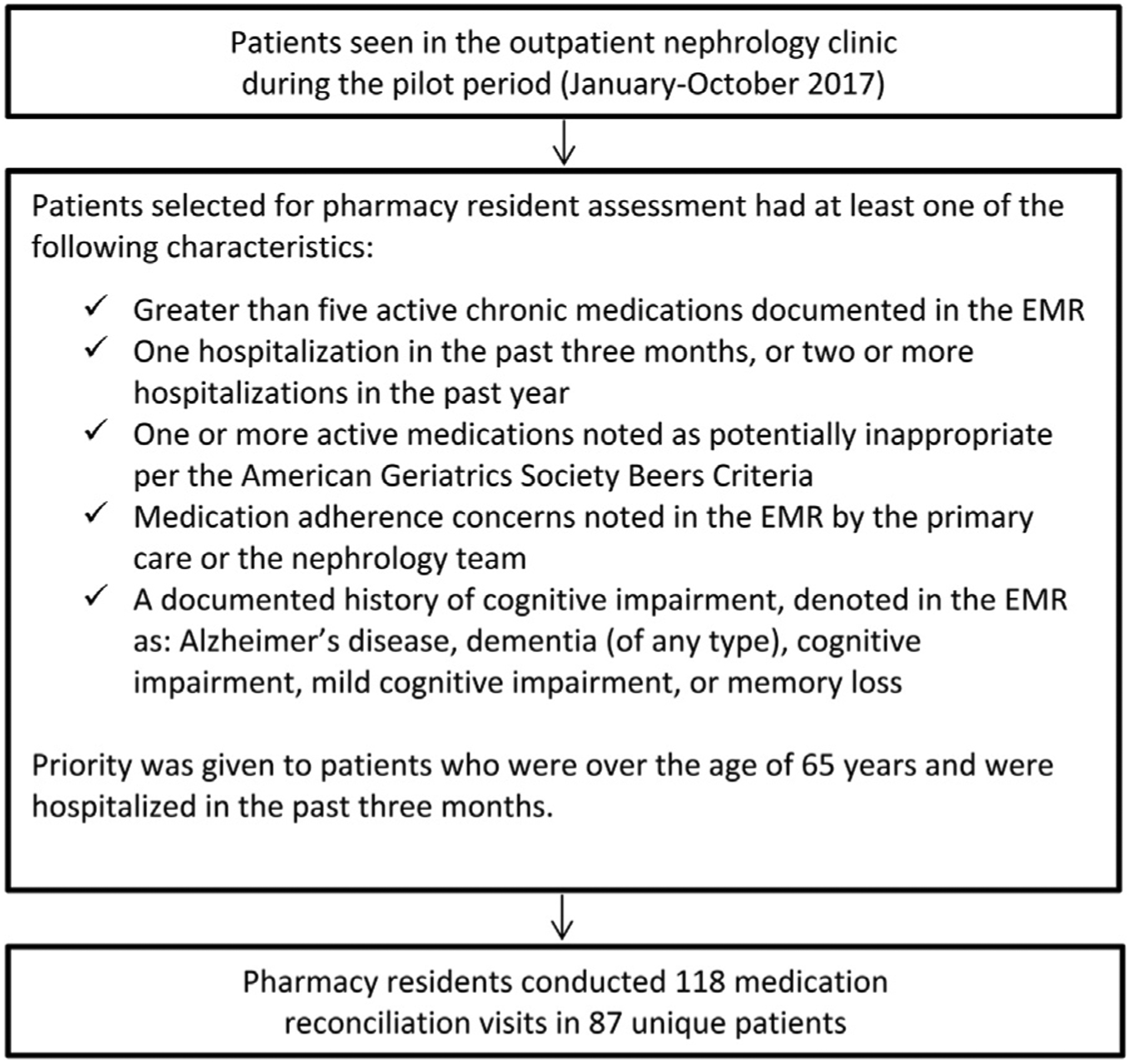
Objectives: To embed pharmacy residents in an interprofessional nephrology clinic to conduct medication reconciliation in targeted high-risk patients with nondialysis kidney disease.
Setting: This pilot was a prospective quality improvement initiative conducted in an interprofessional outpatient nephrology clinic.
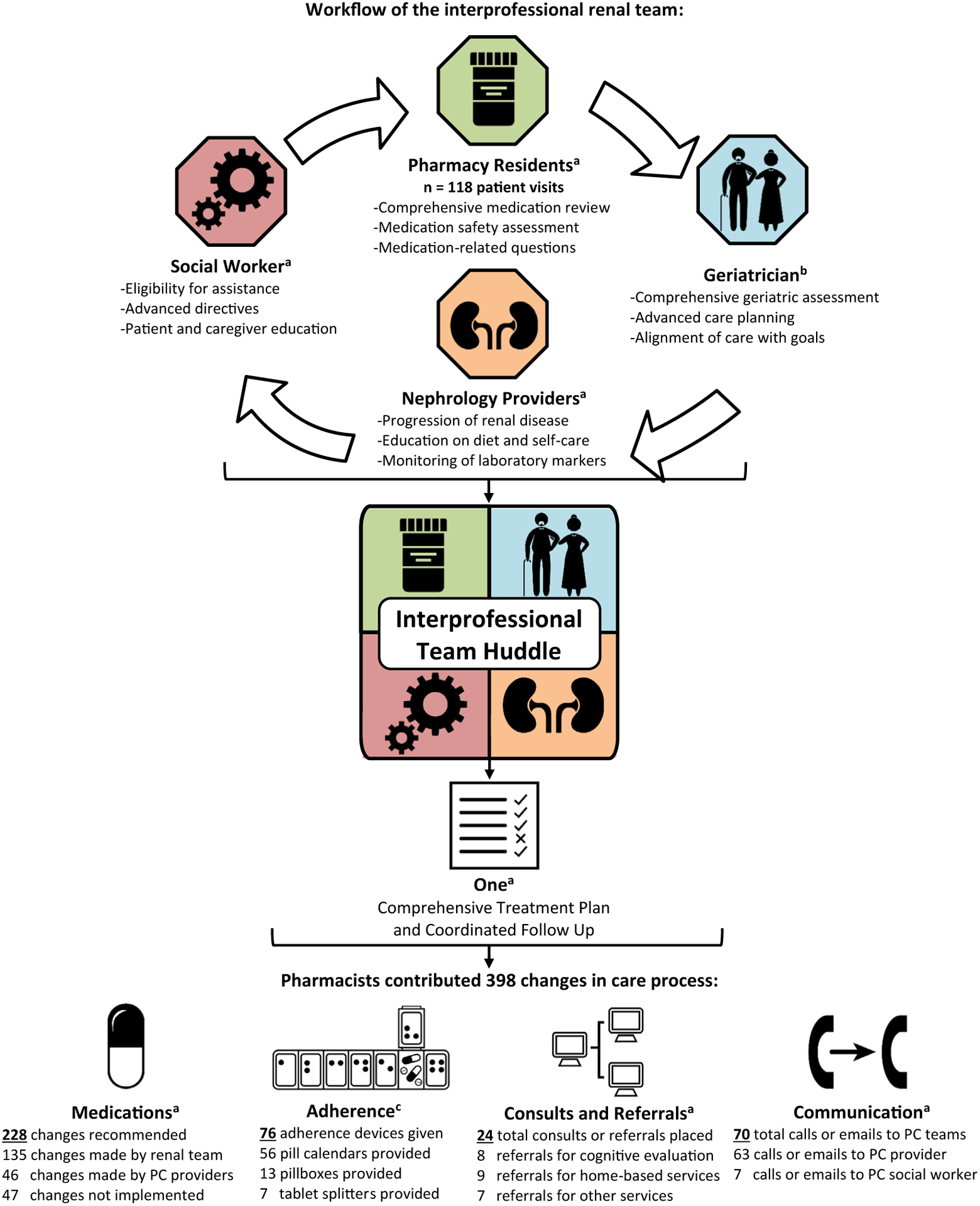
Practice description: The nephrology clinic team includes nephrology providers, a social worker, and a geriatrician. The team is responsible for the management of conditions such as nondialysis kidney disease, resistant hypertension, acute kidney injury, proteinuria, and nephropathy.
Evaluation: Primary outcomes included the number and type of medication discrepancies and drug therapy problems identified. Secondary outcomes included the changes in care process directly resulting from the pharmacy residents' recommendations. The perceived value of the pharmacy residents to the interprofessional team was assessed through postintervention anonymous surveys and semistructured interviews.
Results: The pharmacy residents conducted 118 visits for 87 unique patients (mean age 73 years, 97% male) with nondialysis kidney disease (89% stages III-V), polypharmacy (87% of patients taking > 10 medications), and a heavy comorbidity burden (85% hypertension, 80% dyslipidemia, 59% diabetes mellitus type II) from January to October 2017. Pharmacists identified 344 medication discrepancies and 301 drug therapy problems, resulting in 398 changes in care process. The most frequently identified discrepancies and drug therapy problems were the omission of an active medication from the medication list (86 of 344 discrepancies, 25%) and potentially inappropriate medications (106 of 301 drug therapy problems, 35%). Pharmacists recommended 228 medication changes, provided 76 adherence devices, facilitated 24 consults or referrals, and communicated with the primary care team on 70 occasions. The interprofessional team members all strongly agreed that patients and the team benefited from the pharmacists' involvement.
Conclusion: Pharmacy resident-led medication reconciliation resulted in the identification and resolution of medication discrepancies and drug therapy problems, leading to changes in the care process.
Published by Elsevier Inc.
Conflict of interest statement
Figures
References
-
- Weisberg LS. The patient-centered medical home and the nephrologist. Adv Chronic Kidney Dis. 2011;18:450–455. - PubMed
-
- Rosner M, Abdel-Rahman E, Williams ME. American Society of Nephrology Advisory Group on Geriatric Nephrology. Geriatric nephrology: responding to a growing challenge. Clin J Am Soc Nephrol. 2010;5:936–942. - PubMed
-
- Banerjee G, Karia S, Varley J, Brown EA. Cognitive impairment in elderly renal inpatients: an under-identified phenomenon. Nephron Clin Pract. 2014;126:19–23. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
