

Incidence of New Onset Diabetes Mellitus Secondary to Acute Pancreatitis: A Systematic Review and Meta-Analysis
- PMID: 31231233
- PMCID: PMC6558372
- DOI: 10.3389/fphys.2019.00637
Incidence of New Onset Diabetes Mellitus Secondary to Acute Pancreatitis: A Systematic Review and Meta-Analysis
Abstract
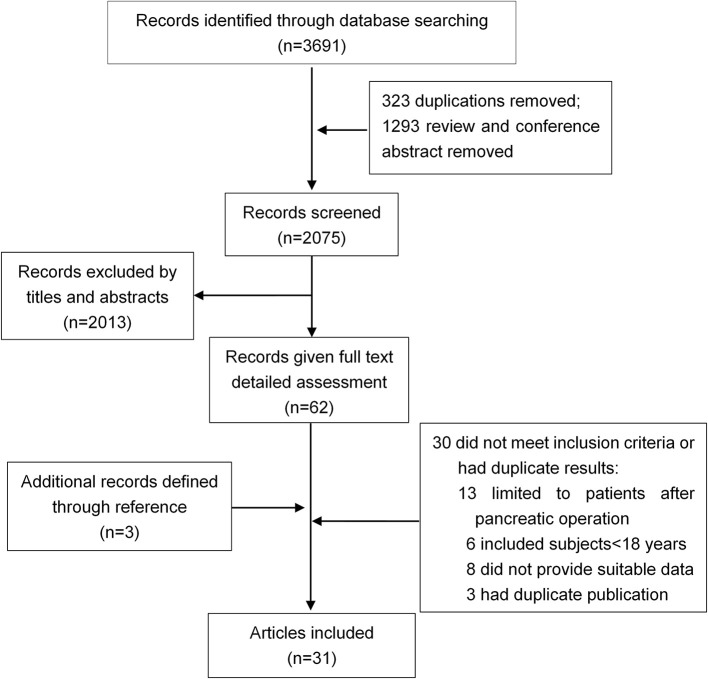
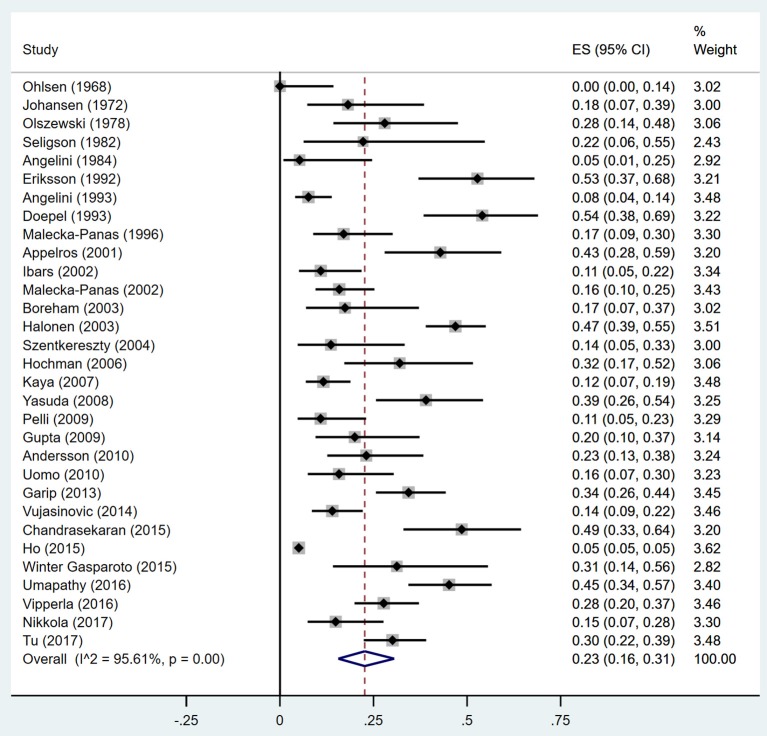
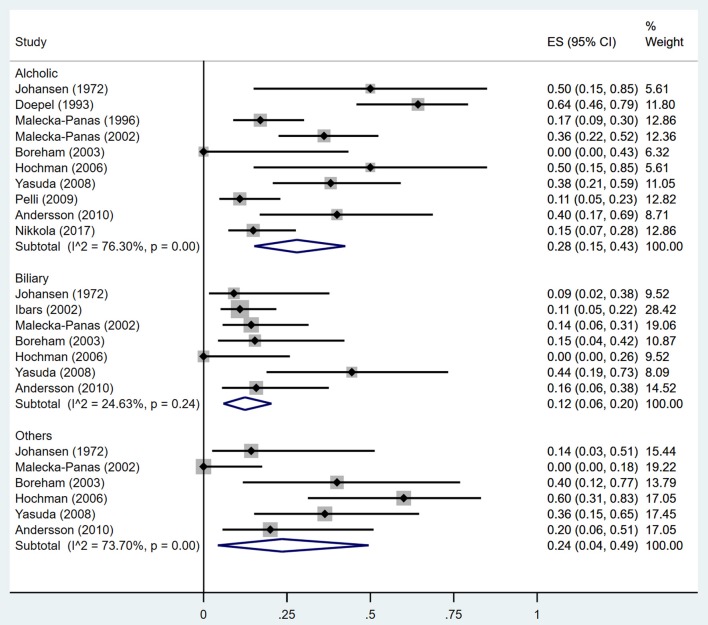
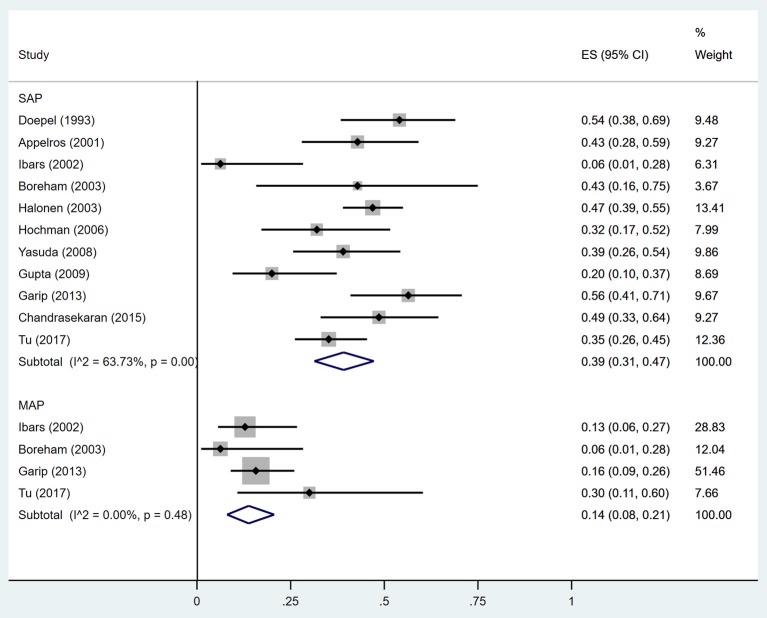
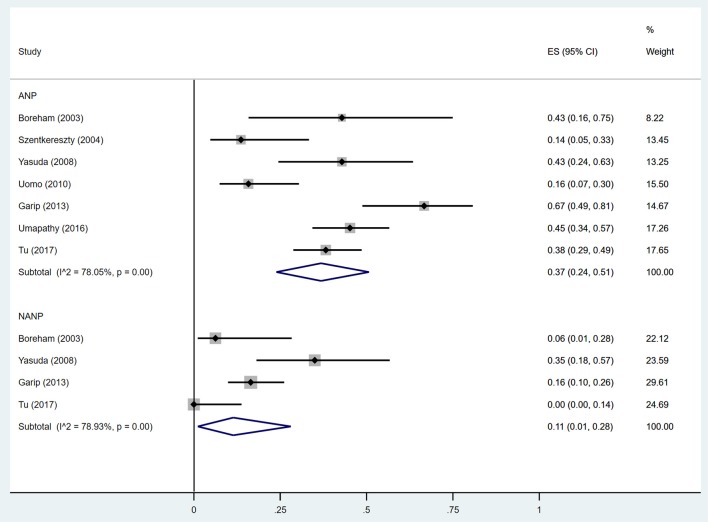
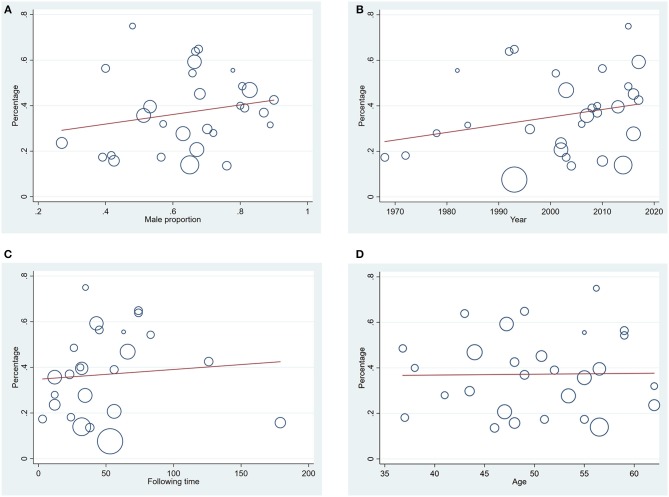
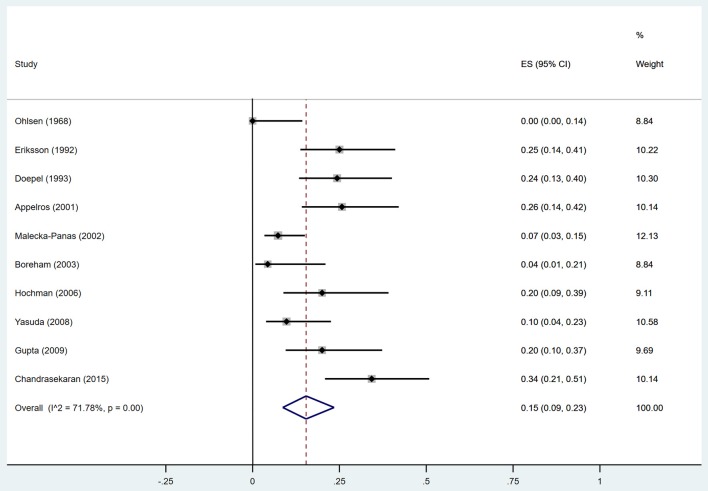
Background and Aims: Patients who have an episode of acute pancreatitis (AP) frequently develop diabetes mellitus (DM) over time. The reported incidence of DM after AP varies depending on the severity, etiology and the extent of pancreatic necrosis during AP. We performed a systematic review to determine the incidence of new-onset DM after AP episode (s), and compared the rate of DM in AP patients based upon different disease characteristics. Methods: A total of 31 relevant studies with 13894 subjects were collected from Medline, Embase, and Web of Science. Stata 15 software was used for data analyses in the meta-analysis. Results: The random-effects pooled incidence was 23.0% for DM (95% CI 16.0-31.0%) and 15.0% (95% CI 9.0-23.0%) for DM treated with insulin. We noted substantial heterogeneity in incidence estimates for DM and DM treated with insulin (I 2 = 95.61 and 71.78%; both p < 0·001). The DM incidence was higher in the populations that had a severe AP (SAP) episode than in those with mild acute pancreatitis (MAP) (39 vs. 14%). Patients that displayed pancreatic necrosis during the AP attack(s) had a higher frequency of DM than those without necrosis (37 vs. 11%). In addition, the pooled incidence of DM was higher after alcoholic compared to biliary AP (28 vs. 12%). The incidence of insulin use after SAP and alcoholic AP was 21 and 18%, respectively, with very low heterogeneities. According to duration of follow-up, the pooled rate of DM and insulin use within 5 years after AP was 20 and 14%, while the rate associated with follow-up duration of more than 5 years was elevated to 37 and 25%, respectively. On meta-regression, year of publication, male proportion, age at DM test, and duration of follow-up were neither positively nor negatively associated with the incidence of DM and DM treated with insulin in patients who had a prior AP attack. Conclusion: Patients with AP developed DM after discharge from hospital with a frequency of about 23%. SAP, alcoholic AP and acute necrotizing pancreatitis (ANP) were associated with increased incidence of DM. Assessments of severity, etiology, and pancreatic necrosis are critical for predicting DM development after AP.
Keywords: acute pancreatitis; diabetes mellitus; etiology; necrosis; severity.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous