

Multi-Institutional Dosimetric Evaluation of Modern Day Stereotactic Radiosurgery (SRS) Treatment Options for Multiple Brain Metastases
- PMID: 31231614
- PMCID: PMC6568036
- DOI: 10.3389/fonc.2019.00483
Multi-Institutional Dosimetric Evaluation of Modern Day Stereotactic Radiosurgery (SRS) Treatment Options for Multiple Brain Metastases
Abstract
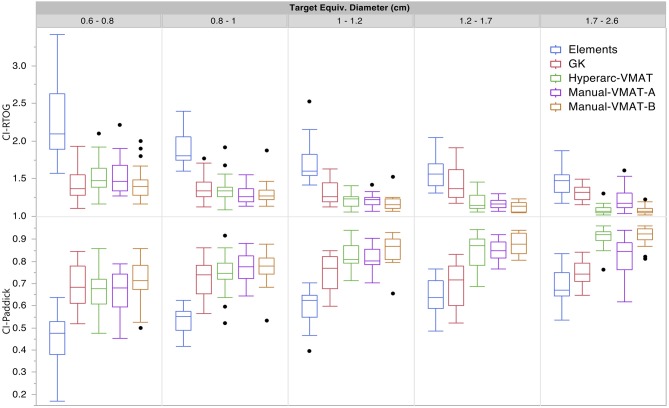
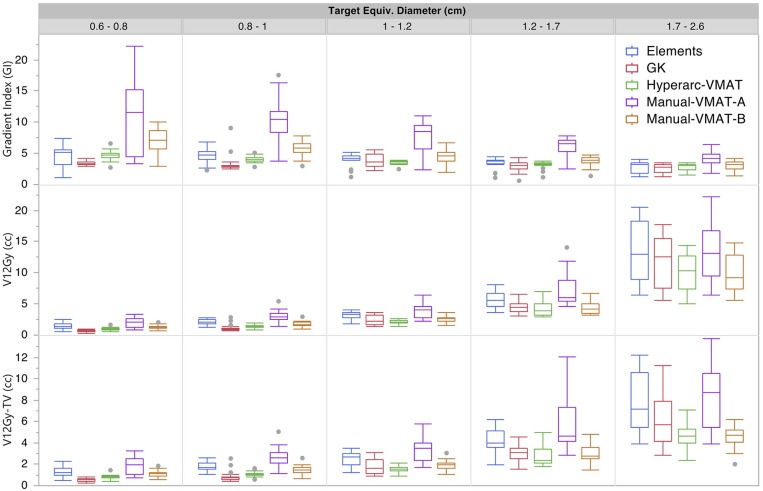
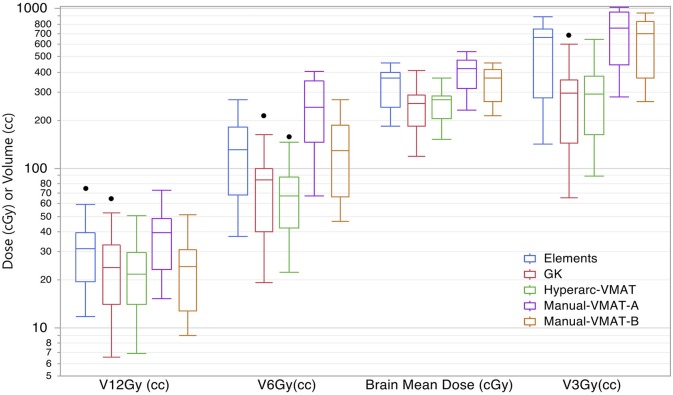
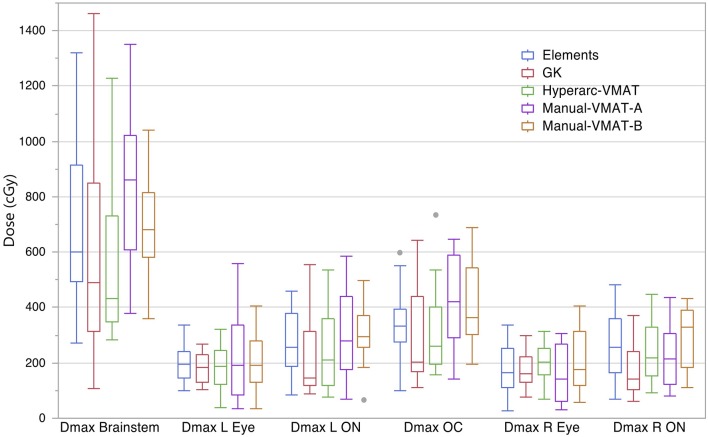
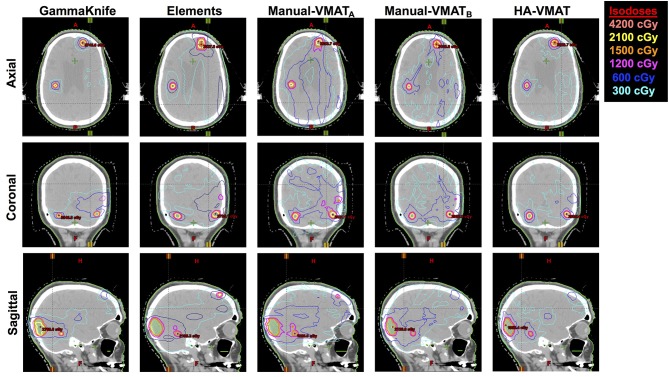
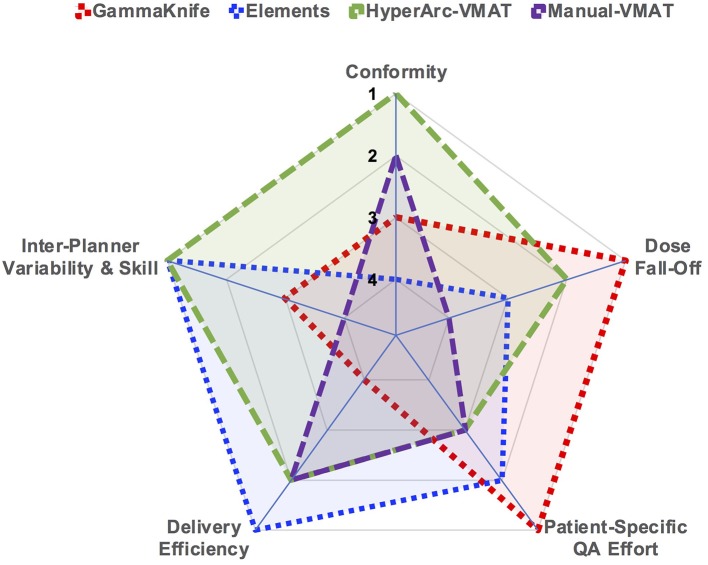
Purpose/Objectives: There are several popular treatment options currently available for stereotactic radiosurgery (SRS) of multiple brain metastases: 60Co sources and cone collimators around a spherical geometry (GammaKnife), multi-aperture dynamic conformal arcs on a linac (BrainLab Elements™ v1.5), and volumetric arc therapy on a linac (VMAT) calculated with either the conventional optimizer or with the Varian HyperArc™ solution. This study aimed to dosimetrically compare and evaluate the differences among these treatment options in terms of dose conformity to the tumor as well as dose sparing to the surrounding normal tissues. Methods and Materials: Sixteen patients and a total of 112 metastases were analyzed. Five plans were generated per patient: GammaKnife, Elements, HyperArc-VMAT, and two Manual-VMAT plans to evaluate different treatment planning styles. Manual-VMAT plans were generated by different institutions according to their own clinical planning standards. The following dosimetric parameters were extracted: RTOG and Paddick conformity indices, gradient index, total volume of brain receiving 12Gy, 6Gy, and 3Gy, and maximum doses to surrounding organs. The Wilcoxon signed rank test was applied to evaluate statistically significant differences (p < 0.05). Results: For targets ≤ 1 cm, GammaKnife, HyperArc-VMAT and both Manual-VMAT plans achieved comparable conformity indices, all superior to Elements. However, GammaKnife resulted in the lowest gradient indices at these target sizes. HyperArc-VMAT performed similarly to GammaKnife for V12Gy parameters. For targets ≥ 1 cm, HyperArc-VMAT and Manual-VMAT plans resulted in superior conformity vs. GammaKnife and Elements. All SRS plans achieved clinically acceptable organs-at-risk dose constraints. Beam-on times were significantly longer for GammaKnife. Manual-VMATA and Elements resulted in shorter delivery times relative to Manual-VMATB and HyperArc-VMAT. Conclusion: The study revealed that Manual-VMAT and HyperArc-VMAT are capable of achieving similar low dose brain spillage and conformity as GammaKnife, while significantly minimizing beam-on time. For targets smaller than 1 cm in diameter, GammaKnife still resulted in superior gradient indices. The quality of the two sets of Manual-VMAT plans varied greatly based on planner and optimization constraint settings, whereas HyperArc-VMAT performed dosimetrically superior to the two Manual-VMAT plans.
Keywords: conformity index; dynamic conformal arcs; multiple brain metastases; stereotactic radiosurgery; volumetric arc therapy.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources