

Prescribing Controversies: An Updated Review and Meta-Analysis on Combined/Alternating Use of Ibuprofen and Paracetamol in Febrile Children
- PMID: 31231621
- PMCID: PMC6560148
- DOI: 10.3389/fped.2019.00217
Prescribing Controversies: An Updated Review and Meta-Analysis on Combined/Alternating Use of Ibuprofen and Paracetamol in Febrile Children
Abstract
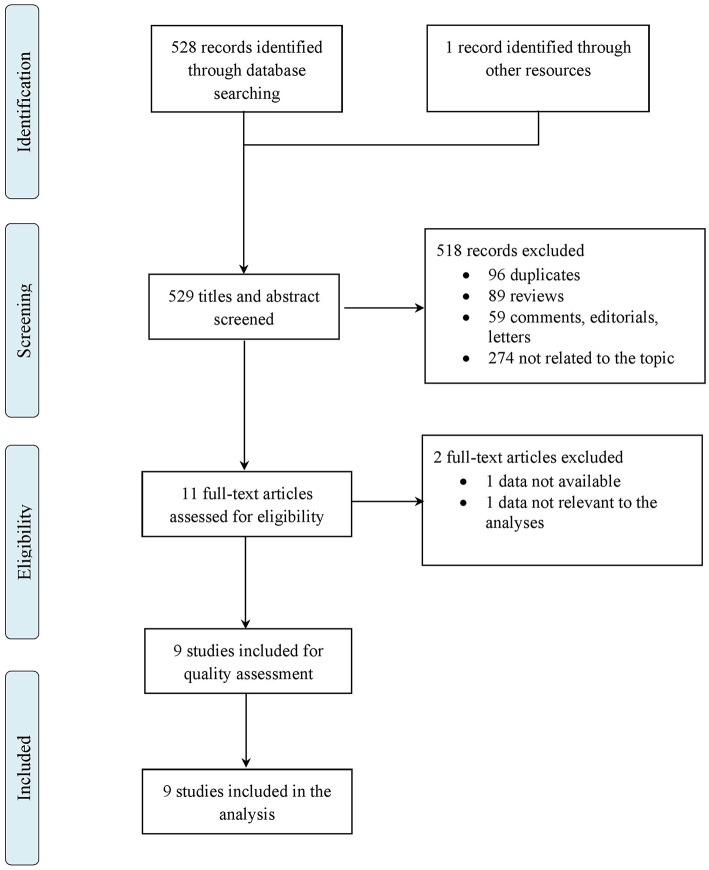
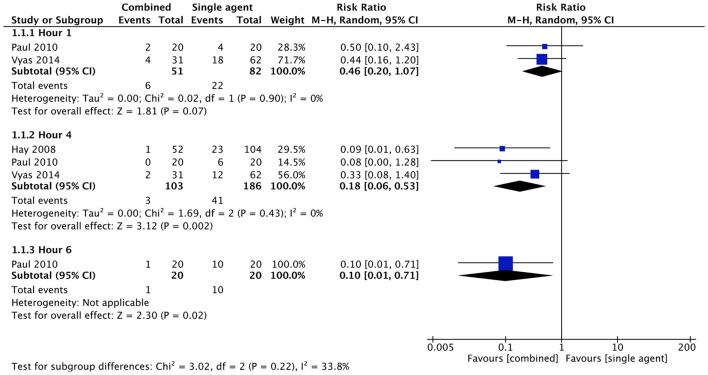
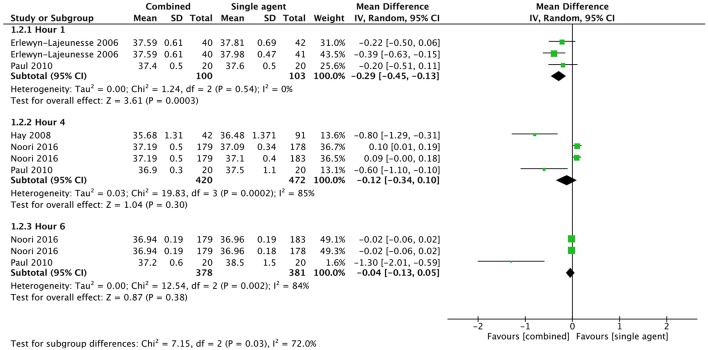
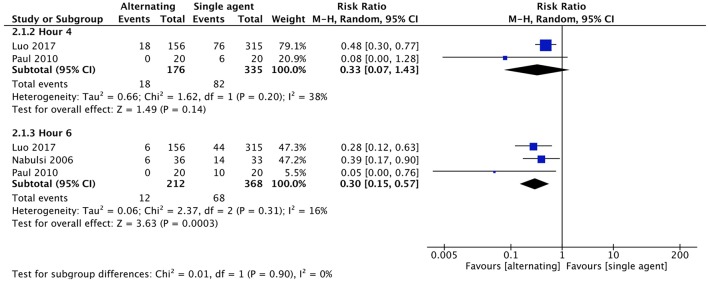
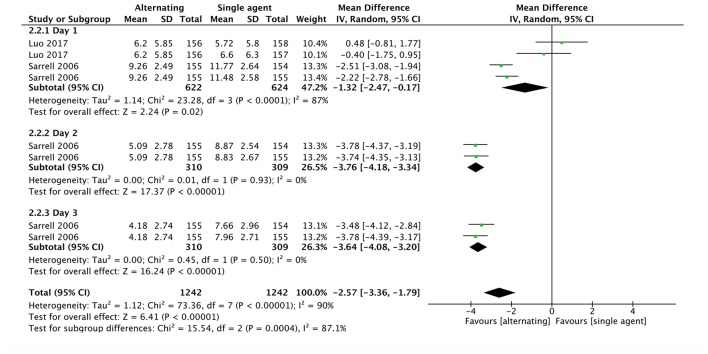
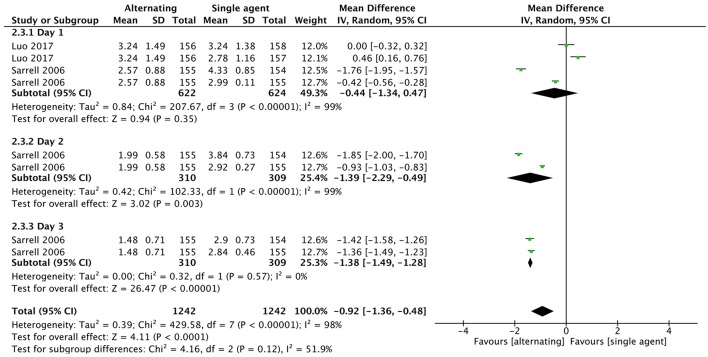
Background: Ibuprofen and paracetamol are the only antipyretics recommended in febrile children. According to international guidelines the choice of the drug should rely on the child's individual characteristics, while a controversial issue regards the combined or alternate use of the two drugs. Objective: To compare the efficacy and safety of combined or alternating use of ibuprofen and paracetamol in children. Methods: A systematic review of literature was performed on Medline and Embase databases. The included studies were randomized controlled trials analyzing the efficacy of combined or alternating therapy with antipyretics in febrile children vs. monotherapy. A meta-analysis was performed to measure the effect of treatment on child's temperature and discomfort. Adverse effects were analyzed as secondary outcome. Results: Nine studies were included, involving 2,026 children. Mean temperature was lower in the combined therapy group at 1 h (mean difference: -0.29°C; 95%CI: -0.45 to -0.13) after the initial administration of therapy. No statistical difference was found in mean temperature at 4 and 6 h from baseline. A significant difference was found in the proportion of children reaching apyrexia at 4 and 6 h with the combined treatment (RR: 0.18, 95%CI: 0.06 to 0.53, and 0.10, 95%CI: 0.01-0.71, respectively) and at 6 h with alternating treatment (RR: 0.30, 95% CI: 0.15-0.57), compared to children treated with monotherapy. The child's discomfort score was slightly lower with alternating therapy vs. monotherapy. The pooled mean difference in the number of medication doses per child used during the first 24 h was not significantly different among groups. Discussion: Combined or alternating therapy resulted more effective than monotherapy in reducing body temperature. However, the benefit appeared modest and probably not clinically relevant. The effect on child discomfort and number of doses of medication was modest as well. According to our findings, evidences are not robust enough to encourage combined or alternating paracetamol and ibuprofen instead of monotherapy to treat febrile children, reinforcing the current recommendation of most of the international guidelines.
Keywords: acetaminophen; antipyretics; children; fever; ibuprofen; paracetamol.
Figures
References
-
- Bertille N, Purssell E, Hjelm N, Bilenko N, Chiappini E, de Bont EGPM, et al. . Symptomatic management of febrile illnesses in children: a systematic review and meta-analysis of parents' knowledge and behaviors and their evolution over time. Front Pediatr. (2018) 6:279. 10.3389/fped.2018.00279 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources