

Intensity-Modulated Proton and Carbon-Ion Radiation Therapy in the Management of Head and Neck Sarcomas
- PMID: 31231939
- PMCID: PMC6712452
- DOI: 10.1002/cam4.2319
Intensity-Modulated Proton and Carbon-Ion Radiation Therapy in the Management of Head and Neck Sarcomas
Abstract
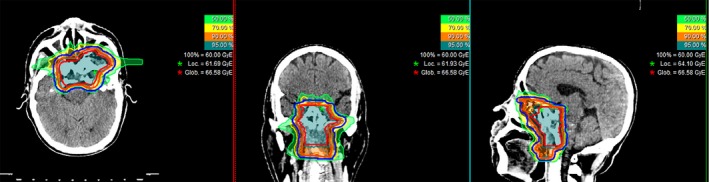
Purpose: We report our experience of intensity-modulated proton and carbon-ion radiotherapy (IMPT/IMCT) for head and neck sarcomas (HNS).
Methods and materials: An analysis of the ongoing prospective data registry from the Shanghai Proton and Heavy Ion Center (SPHIC) for patients with HNS was conducted. The 12- and 24-month rates of local recurrence-free, overall, distant metastasis-free, progression-free survival (LRFS, OS, DMFS, and PFS), and acute/late toxicities were calculated. The prognostic factors for the effectiveness of the treatment were also analyzed.
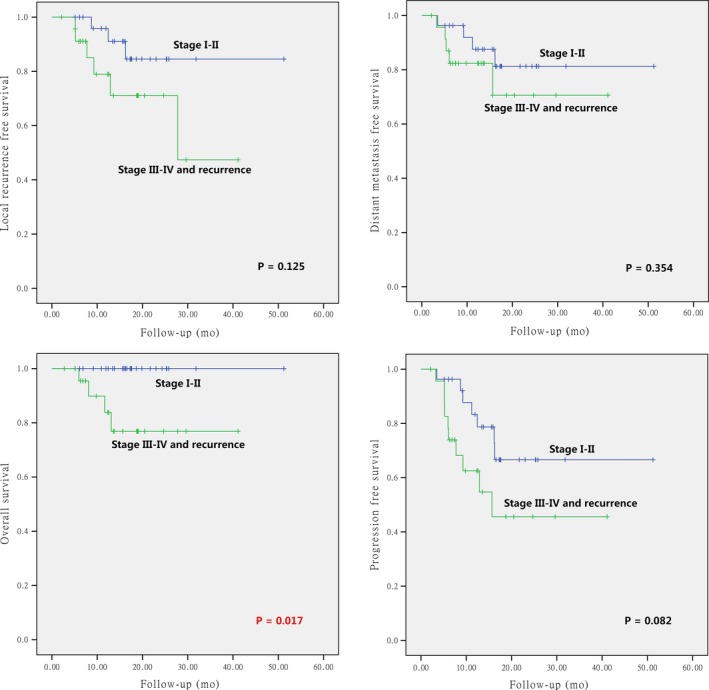
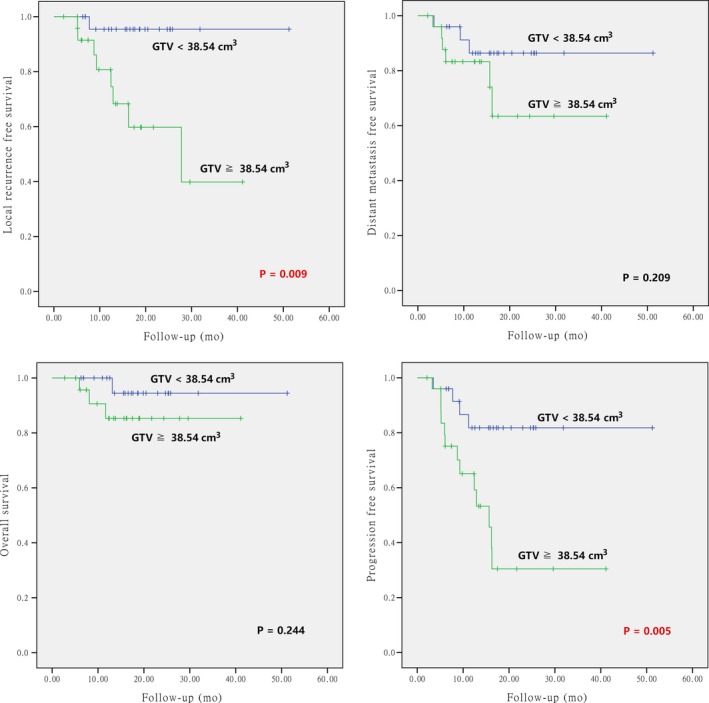
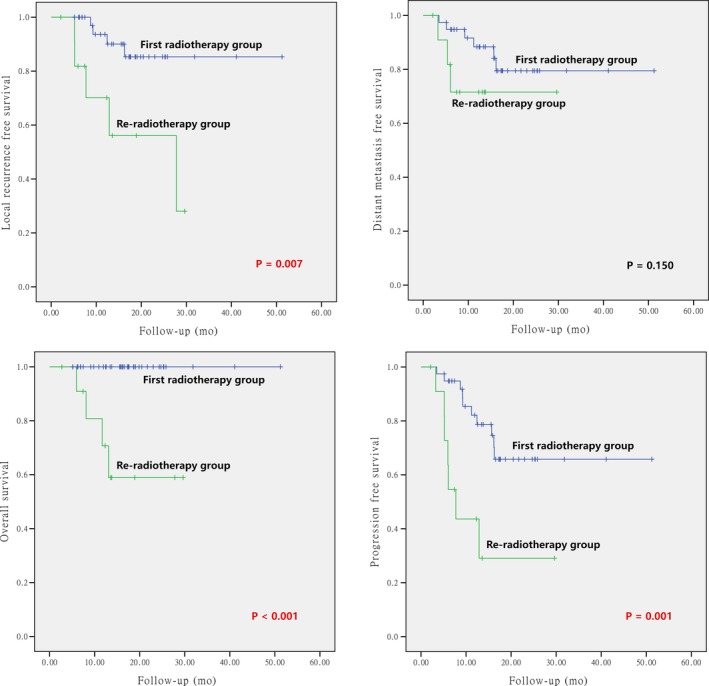
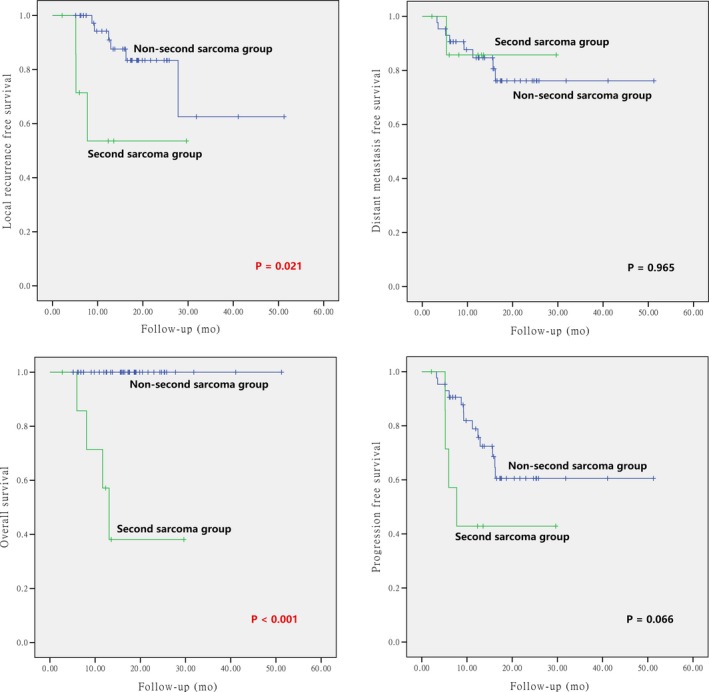
Results: Between 7/2014 and 5/2018, 51 consecutive patients with HNS received definitive doses of IMCT (41 cases), IMPT (two cases), or their combination (eight cases). One patient had R0 resection and another treated on the Chinese Food and Drug Administration registration trial received IMPT only. Twenty-seven patients were treated according to various dose escalation trials or institutional protocols using IMCT or IMPT + IMCT boost. Twenty-two patients with locoregional recurrence (10 and four patients failed surgery or surgery followed by radiotherapy, respectively) or radiation-induced second primary sarcomas (eight patients) received salvage particle radiotherapy. With a median follow-up time of 15.7 months, four patients with second primary sarcoma died. The 1- and 2-year OS, PFS, LRFS, and DMFS rates for the entire cohort were 92.9% vs 90%, 73.6% vs 57.4%, 88.4% vs 78.9%, and 84.6% vs 76.5%, respectively. Those rates for patients without prior radiotherapy were 100% vs 100%, 82.1% vs 65.8%, 93.6% vs 85.3%, and 88.4% vs 79.5%, respectively. Multivariate analyses revealed that re-irradiation was an independent prognostic factor for both LRFS and PFS (P = 0.015 and 0.037, respectively). In addition, gross tumor volume (GTV) was an independent prognostic factor for PFS (P = 0.048). One patient experienced Grade 3 acute toxicity (oral mucositis); another experienced Grade 4 acute event (hemorrhage) which required embolization. He lately died from hemorrhage (Grade 5) at 3.4 months after the completion of treatment. No patient experienced radiation-induced acute/late toxicity of ≥ Grade 2 otherwise.
Conclusion: With few observed acute/late toxicities, IMPT/IMCT provided effective short-term tumor control in our patients with HNS. Further investigations, preferably in a prospective fashion, will be required to confirm the efficacy and toxicities of IMPT/IMCT in this group of patients.
© 2019 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors have declared that no competing interest exists.
Figures
References
-
- Farhood AI, Hajdu SI, Shiu MH, Strong EW. Soft tissue sarcomas of the head and neck in adults. Am J Surg. 1990;160(4):365‐369. - PubMed
-
- Chen SA, Morris CG, Amdur RJ, Werning JW, Villaret DB, Mendenhall WM. Adult Head and Neck Soft Tissue Sarcomas. Am J Clin Oncol. 2005;28(3):259‐263. - PubMed
-
- Mendenhall WM, Mendenhall CM, Werning JW, Riggs CE, Mendenhall NP. Adult head and neck soft tissue sarcomas. Head Neck. 2005;27(10):916‐922. - PubMed
-
- Huber GF, Matthews TW, Dort JC. Soft‐tissue sarcomas of the head and neck: a retrospective analysis of the Alberta experience 1974 to 1999. The Laryngoscope. 2006;116(5):780‐785. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
