

Efficacy of Home-Based Telerehabilitation vs In-Clinic Therapy for Adults After Stroke: A Randomized Clinical Trial
- PMID: 31233135
- PMCID: PMC6593624
- DOI: 10.1001/jamaneurol.2019.1604
Efficacy of Home-Based Telerehabilitation vs In-Clinic Therapy for Adults After Stroke: A Randomized Clinical Trial
Abstract
Importance: Many patients receive suboptimal rehabilitation therapy doses after stroke owing to limited access to therapists and difficulty with transportation, and their knowledge about stroke is often limited. Telehealth can potentially address these issues.
Objectives: To determine whether treatment targeting arm movement delivered via a home-based telerehabilitation (TR) system has comparable efficacy with dose-matched, intensity-matched therapy delivered in a traditional in-clinic (IC) setting, and to examine whether this system has comparable efficacy for providing stroke education.
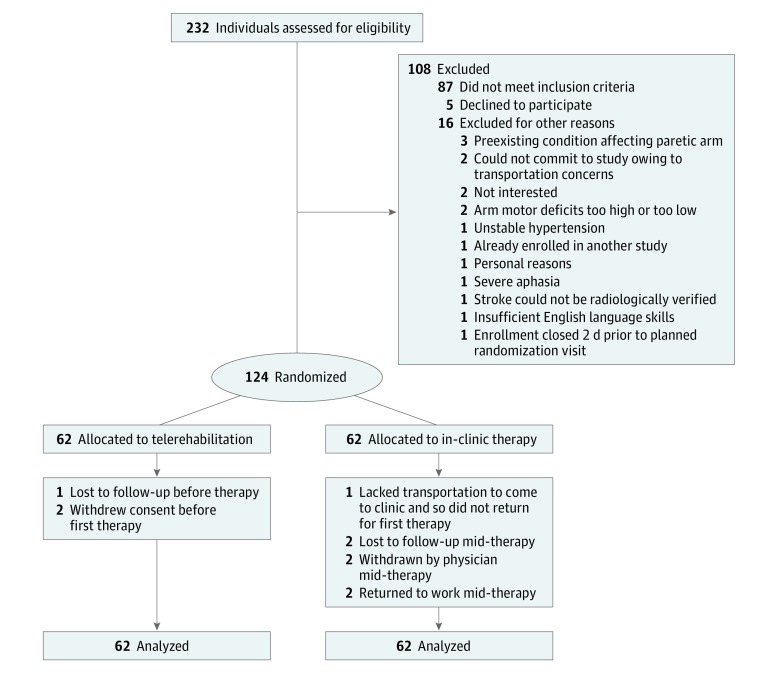
Design, setting, and participants: In this randomized, assessor-blinded, noninferiority trial across 11 US sites, 124 patients who had experienced stroke 4 to 36 weeks prior and had arm motor deficits (Fugl-Meyer [FM] score, 22-56 of 66) were enrolled between September 18, 2015, and December 28, 2017, to receive telerehabilitation therapy in the home (TR group) or therapy at an outpatient rehabilitation therapy clinic (IC group). Primary efficacy analysis used the intent-to-treat population.
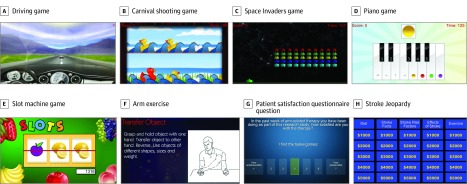
Interventions: Participants received 36 sessions (70 minutes each) of arm motor therapy plus stroke education, with therapy intensity, duration, and frequency matched across groups.
Main outcomes and measures: Change in FM score from baseline to 4 weeks after end of therapy and change in stroke knowledge from baseline to end of therapy.
Results: A total of 124 participants (34 women and 90 men) had a mean (SD) age of 61 (14) years, a mean (SD) baseline FM score of 43 (8) points, and were enrolled a mean (SD) of 18.7 (8.9) weeks after experiencing a stroke. Among those treated, patients in the IC group were adherent to 33.6 of the 36 therapy sessions (93.3%) and patients in the TR group were adherent to 35.4 of the 36 assigned therapy sessions (98.3%). Patients in the IC group had a mean (SD) FM score change of 8.36 (7.04) points from baseline to 30 days after therapy (P < .001), while those in the TR group had a mean (SD) change of 7.86 (6.68) points (P < .001). The covariate-adjusted mean FM score change was 0.06 (95% CI, -2.14 to 2.26) points higher in the TR group (P = .96). The noninferiority margin was 2.47 and fell outside the 95% CI, indicating that TR is not inferior to IC therapy. Motor gains remained significant when patients enrolled early (<90 days) or late (≥90 days) after stroke were examined separately.
Conclusions and relevance: Activity-based training produced substantial gains in arm motor function regardless of whether it was provided via home-based telerehabilitation or traditional in-clinic rehabilitation. The findings of this study suggest that telerehabilitation has the potential to substantially increase access to rehabilitation therapy on a large scale.
Trial registration: ClinicalTrials.gov identifier: NCT02360488.
Conflict of interest statement
Figures
Comment in
-
Critically appraised paper: Upper limb post-stroke telerehabilitation is not inferior to in-clinic rehabilitation.J Physiother. 2020 Jul;66(3):198. doi: 10.1016/j.jphys.2020.05.002. Epub 2020 Jul 10. J Physiother. 2020. PMID: 32660914 No abstract available.
-
Critically appraised paper: Upper limb post-stroke telerehabilitation is not inferior to in-clinic rehabilitation [commentary].J Physiother. 2020 Jul;66(3):198. doi: 10.1016/j.jphys.2020.05.001. Epub 2020 Jul 14. J Physiother. 2020. PMID: 32680740 No abstract available.
References
-
- Winstein CJ, Stein J, Arena R, et al. ; American Heart Association Stroke Council, Council on Cardiovascular and Stroke Nursing, Council on Clinical Cardiology, and Council on Quality of Care and Outcomes Research . Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2016;47(6):e98-e169. doi: 10.1161/STR.0000000000000098 - DOI - PubMed
