

Differences in Advance Care Planning and Circumstances of Death for Pediatric Patients Who Do and Do Not Receive Palliative Care Consults: A Single-Center Retrospective Review of All Pediatric Deaths from 2012 to 2016
- PMID: 31233350
- PMCID: PMC6998041
- DOI: 10.1089/jpm.2019.0111
Differences in Advance Care Planning and Circumstances of Death for Pediatric Patients Who Do and Do Not Receive Palliative Care Consults: A Single-Center Retrospective Review of All Pediatric Deaths from 2012 to 2016
Abstract
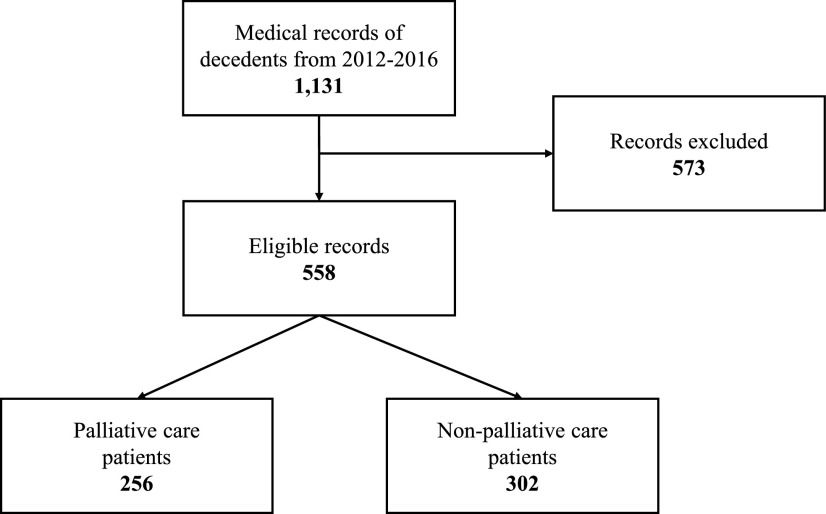
Background: Growing evidence suggests that pediatric palliative care (PPC) teams influence the care received by children and young adults with chronic, life-limiting illnesses. Little is known about how PPC involvement affects advance care planning (ACP) and circumstances of death in pediatric populations with a wide range of diagnoses. Objective: To determine the relationship between PPC involvement, ACP, and circumstances of death for pediatric patients. Design: A retrospective chart review of 558 pediatric patients who died between January 1, 2012 and December 31, 2016 was conducted. Descriptive statistics were used to characterize the sample. A multivariable logistic regression was used to obtain associations between PPC involvement and ACP. Setting: Large, multidisciplinary tertiary care center in a rural state. Measurements: Data abstracted for each patient included the following: demographic information, diagnosis, location of primary unit, hospice involvement, goals of care (GOC), code status, Physician Orders for Life-Sustaining Treatment (POLST) completion, and location of death. Results: Patients with PPC involvement were more likely to have had ACP addressed before death. After adjusting for covariates in the model, patients with PPC were more likely to have their GOC documented (odds ratio [OR] = 96.93), completion of POLST (OR = 24.06), do-not-resuscitate code status (OR = 7.71), and hospice involvement at the time of death (OR = 11.70) compared with those who did not receive PPC. Conclusions: Pediatric patients are more likely to have ACP addressed if they have PPC involvement. Patients with chronic complex conditions are most likely to receive palliative care.
Keywords: Physician Orders for Life-Sustaining Treatment; advance care planning; death location; pediatric palliative care.
Conflict of interest statement
No competing financial interests exist.
Figures
Similar articles
-
The Impact of Pediatric Palliative Care Involvement in the Care of Critically Ill Patients without Complex Chronic Conditions.J Palliat Med. 2019 May;22(5):553-556. doi: 10.1089/jpm.2018.0469. Epub 2018 Dec 27. J Palliat Med. 2019. PMID: 30589623
-
The impact of specialized pediatric palliative care on advance care planning and healthcare utilization in children and young adults: a retrospective analysis of medical records of in-hospital deaths.BMC Palliat Care. 2024 May 22;23(1):127. doi: 10.1186/s12904-024-01448-w. BMC Palliat Care. 2024. PMID: 38778335 Free PMC article.
-
Early Versus Late Outpatient Pediatric Palliative Care Consultation and Its Association With End-of-Life Outcomes in Children With Cancer.J Palliat Med. 2023 Nov;26(11):1466-1473. doi: 10.1089/jpm.2023.0063. Epub 2023 May 24. J Palliat Med. 2023. PMID: 37222727
-
Are We on the Same Page? Exploring Pediatric Patients' Involvement With Advance Care Planning.J Pain Symptom Manage. 2023 Sep;66(3):e353-e363. doi: 10.1016/j.jpainsymman.2023.04.003. Epub 2023 Apr 11. J Pain Symptom Manage. 2023. PMID: 37054956 Review.
-
Pediatric Palliative Care.Hosp Pract (1995). 2021 Oct;49(sup1):422-430. doi: 10.1080/21548331.2021.1964867. Epub 2021 Sep 3. Hosp Pract (1995). 2021. PMID: 34346272 Review.
Cited by
-
Stories of paediatric palliative care: a qualitative study exploring health care professionals' understanding of the concept.BMC Palliat Care. 2022 Oct 22;21(1):187. doi: 10.1186/s12904-022-01077-1. BMC Palliat Care. 2022. PMID: 36273144 Free PMC article.
-
Bereaved parents' perspectives on their child's end-of-life care: connecting a self-report questionnaire and interview data from the nationwide Paediatric End-of-LIfe CAre Needs in Switzerland (PELICAN) study.BMC Palliat Care. 2022 May 4;21(1):66. doi: 10.1186/s12904-022-00957-w. BMC Palliat Care. 2022. PMID: 35509046 Free PMC article.
-
Interventions Performed in Children With Immunocompromised Conditions in the Pediatric Intensive Care Unit Within 48 Hours of Death.J Palliat Med. 2024 May;27(5):644-650. doi: 10.1089/jpm.2023.0400. Epub 2024 Jan 17. J Palliat Med. 2024. PMID: 38232707 Free PMC article.
-
Barriers and facilitators influencing referral and access to palliative care for children and young people with life-limiting and life-threatening conditions: a scoping review of the evidence.Palliat Med. 2024 Oct;38(9):981-999. doi: 10.1177/02692163241271010. Epub 2024 Sep 9. Palliat Med. 2024. PMID: 39248205 Free PMC article.
-
Advance Care Planning in Serious Illness: A Narrative Review.J Pain Symptom Manage. 2023 Jan;65(1):e63-e78. doi: 10.1016/j.jpainsymman.2022.08.012. Epub 2022 Aug 24. J Pain Symptom Manage. 2023. PMID: 36028176 Free PMC article. Review.
References
-
- Feudtner C, Friebert S, Jewell J: Policy statement: Pediatric palliative care and hospice care commitments, guidelines, and recommendations. Pediatrics 2013;132:966–972 - PubMed
-
- Widger K, Sutradhar R, Rapoport A, et al. : Predictors of specialized pediatric palliative care involvement and impact on patterns of end-of-life care in children with cancer. J Clin Oncol 2018;36:801–807 - PubMed
-
- Feudtner C, Womer J, Augustin R, et al. : Pediatric palliative care programs in children's hospitals: A cross-sectional national survey. Pediatrics 2013;132:1063–1070 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
