

Impact of Teratoma on the Cumulative Incidence of Disease-Related Death in Patients With Advanced Germ Cell Tumors
- PMID: 31233353
- PMCID: PMC7001787
- DOI: 10.1200/JCO.18.01608
Impact of Teratoma on the Cumulative Incidence of Disease-Related Death in Patients With Advanced Germ Cell Tumors
Abstract
Purpose: In men with metastatic germ cell tumors (GCTs), risk-directed treatment is determined, in part, by a distinction between seminoma and nonseminomatous GCT (NSGCT). The importance of NSGCT cell type is uncertain. We evaluated the long-term impact of teratoma on survival in patients with NSGCT.
Methods: Prechemotherapy, primary tumors from patients who received platinum-based chemotherapy were studied, and the histology was confirmed by a genitourinary pathologist. The cumulative incidence of disease-related death (CIDD) was the primary end point, and a competing-risk analysis was performed.
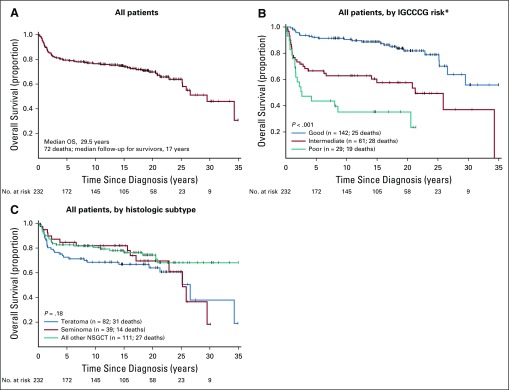
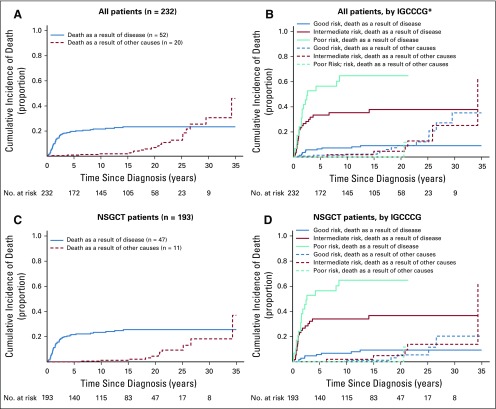
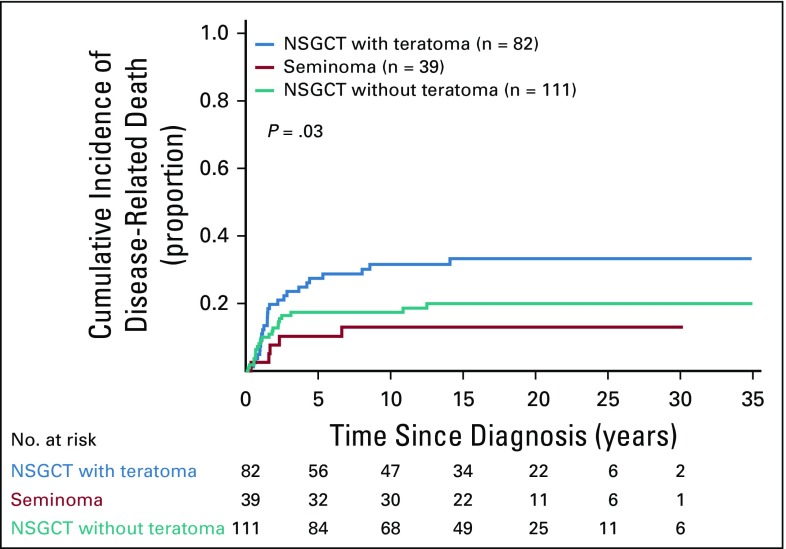
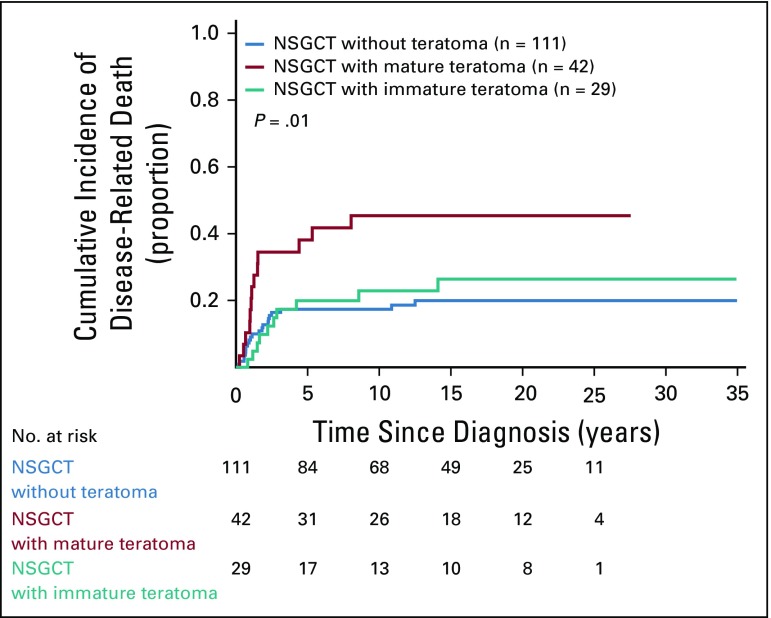
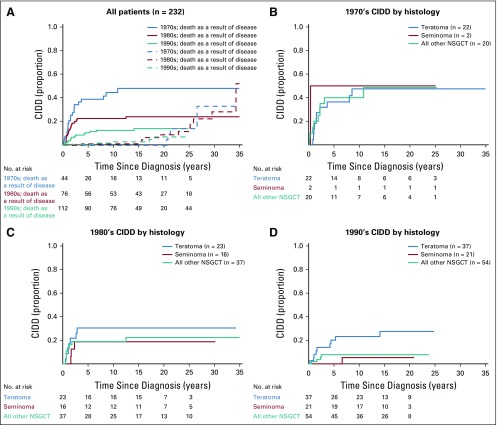
Results: Tumors were available from 232 patients, including 193 with NSGCT. An element of teratoma was present in 82 NSGCT primary tumors (42%). With a median follow-up of 17 years (range, 0.3 to 35 years), 58 patients with NSGCT died, 47 as a result of GCT and 11 as a result of other causes. Most GCT deaths occurred within the first 5 years and were associated with pretreatment risk status (P < .001). Death as a result of other causes rose steadily after 15 years and was not associated with risk status (P = .66). A higher CIDD was observed in patients who had NSGCT with teratoma than those with NSGCT without teratoma and seminoma (5-year CIDD rate, 27.4%, 17.4%, and 10.3%, respectively; P = .03). A higher CIDD was observed in patients who had NSGCT with mature teratoma compared with those with either NSGCT with immature teratoma or NSGCT without teratoma (5-year CIDD rate, 38.1%, 19.9%, and 17.4%, respectively; P = .01).
Conclusion: The presence of teratoma, particularly mature teratoma, in an NSGCT primary tumor is associated with a higher CIDD, consistent with the hypothesis that differentiation is associated with adverse outcomes. Death as a result of non-GCT causes is not associated with risk status and must be separated from GCT death when evaluating long-term survival.
Figures
Comment in
-
Improving the Prognostic Ability for Personalized Therapeutic Approaches in Nonseminomatous Germ Cell Tumors.J Clin Oncol. 2019 Sep 10;37(26):2314-2316. doi: 10.1200/JCO.19.01672. Epub 2019 Jul 30. J Clin Oncol. 2019. PMID: 31361537 No abstract available.
References
-
- Nigam M, Aschebrook-Kilfoy B, Shikanov S, et al. Increasing incidence of testicular cancer in the United States and Europe between 1992 and 2009. World J Urol. 2015;33:623–631. - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Funt SA, Feldman DR, Bosl GJ: The Management of advanced germ cell tumors in 2016: The Memorial Sloan Kettering approach. Oncology (Williston Park) 30:653-664, 2016. - PubMed
-
- Hanna N, Einhorn LH. Testicular cancer: A reflection on 50 years of discovery. J Clin Oncol. 2014;32:3085–3092. - PubMed
-
- Santagata S, Ligon KL, Hornick JL. Embryonic stem cell transcription factor signatures in the diagnosis of primary and metastatic germ cell tumors. Am J Surg Pathol. 2007;31:836–845. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
