

Gaucher Disease in Bone: From Pathophysiology to Practice
- PMID: 31233632
- PMCID: PMC6852006
- DOI: 10.1002/jbmr.3734
Gaucher Disease in Bone: From Pathophysiology to Practice
Abstract
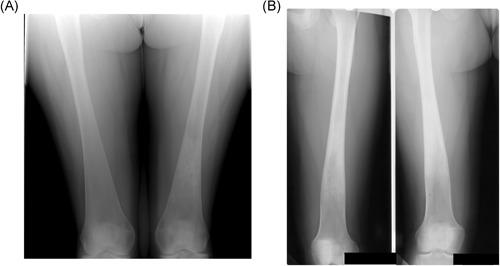
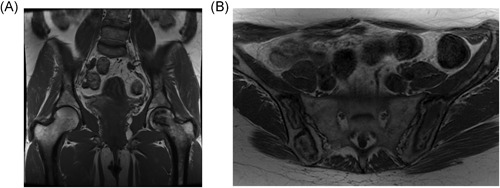
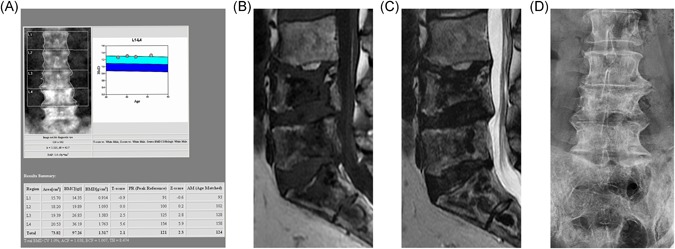
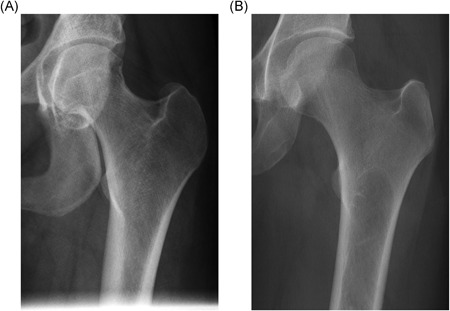
Gaucher disease (GD) is a rare, genetic lysosomal disorder leading to lipid accumulation and dysfunction in multiple organs. Involvement of the skeleton is one of the most prevalent aspects of GD and a major cause of pain, disability, and reduced quality of life. Uniform recommendations for contemporary evaluation and management are needed. To develop practical clinical recommendations, an international group of experienced physicians conducted a comprehensive review of 20 years' of the literature, defining terms according to pathophysiological understanding and pointing out best practice and unmet needs related to the skeletal features of this disorder. Abnormalities of bone modeling, reduced bone density, bone infarction, and plasma cell dyscrasias accompany the displacement of healthy adipocytes in adult marrow. Exposure to excess bioactive glycosphingolipids appears to affect hematopoiesis and the balance of osteoblast and osteoclast numbers and activity. Imbalance between bone formation and breakdown induces disordered trabecular and cortical bone modeling, cortical bone thinning, fragility fractures, and osteolytic lesions. Regular assessment of bone mineral density, marrow infiltration, the axial skeleton and searching for potential malignancy are recommended. MRI is valuable for monitoring skeletal involvement: It provides semiquantitative assessment of marrow infiltration and the degree of bone infarction. When MRI is not available, monitoring of painful acute bone crises and osteonecrosis by plain X-ray has limited value. In adult patients, we recommend DXA of the lumbar spine and left and right hips, with careful protocols designed to exclude focal disease; serial follow-up should be done using the same standardized instrument. Skeletal health may be improved by common measures, including adequate calcium and vitamin D and management of pain and orthopedic complications. Prompt initiation of specific therapy for GD is crucial to optimizing outcomes and preventing irreversible skeletal complications. Investing in safe, clinically useful, and better predictive methods for determining bone integrity and fracture risk remains a need. © 2019 The Authors. Journal of Bone and Mineral Research Published by Wiley Periodicals Inc.
Keywords: BIOMARKERS; BONE DISEASE; GAUCHER DISEASE; OSTEONECROSIS; OSTEOPOROSIS; RADIOLOGY; THERAPEUTICS.
© 2019 The Authors. Journal of Bone and Mineral Research Published by Wiley Periodicals Inc.
Figures


References
-
- Hruska KS, LaMarca ME, Sidransky E Gaucher disease: molecular biology and genotype–phenotype correlations In: Futerman AH, & Zimran A, editors, Gaucher disease. Volume 1. Boca Raton, FL: CRC Press, 2007. Chapter 2, p.13.
-
- Altarescu G, Hill S, Wiggs E, et al. The efficacy of enzyme replacement therapy in patients with chronic neuronopathic Gaucher's disease. J Pediatr. 2001;138(4):539–47. - PubMed
-
- Davies EH, Erikson A, Collin‐Histed T, et al. Outcome of type III Gaucher disease on enzyme replacement therapy: Review of 55 cases. J Inherit Metab Dis. 2007;30(6):935–42. - PubMed
