

Bone-Forming and Antiresorptive Effects of Romosozumab in Postmenopausal Women With Osteoporosis: Bone Histomorphometry and Microcomputed Tomography Analysis After 2 and 12 Months of Treatment
- PMID: 31233639
- PMCID: PMC7027577
- DOI: 10.1002/jbmr.3735
Bone-Forming and Antiresorptive Effects of Romosozumab in Postmenopausal Women With Osteoporosis: Bone Histomorphometry and Microcomputed Tomography Analysis After 2 and 12 Months of Treatment
Abstract
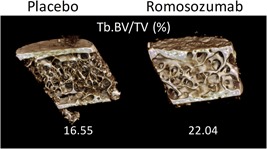
Sclerostin, a protein produced by osteocytes, inhibits bone formation. Administration of sclerostin antibody results in increased bone formation in multiple animal models. Romosozumab, a humanized sclerostin antibody, has a dual effect on bone, transiently increasing serum biochemical markers of bone formation and decreasing serum markers of bone resorption, leading to increased BMD and reduction in fracture risk in humans. We aimed to evaluate the effects of romosozumab on bone tissue. In a subset of 107 postmenopausal women with osteoporosis in the multicenter, international, randomized, double-blind, placebo-controlled Fracture Study in Postmenopausal Women with Osteoporosis (FRAME), transiliac bone biopsies were performed either after 2 (n = 34) or 12 (n = 73) months of treatment with 210 mg once monthly of romosozumab or placebo to evaluate histomorphometry and microcomputed tomography-based microarchitectural endpoints. After 2 months, compared with either baseline values assessed after a quadruple fluorochrome labeling or placebo, significant increases (P < 0.05 to P < 0.001) in dynamic parameters of formation (median MS/BS: romosozumab 1.51% and 5.64%; placebo 1.60% and 2.31% at baseline and month 2, respectively) were associated with a significant decrease compared with placebo in parameters of resorption in cancellous (median ES/BS: placebo 3.4%, romosozumab 1.8%; P = 0.022) and endocortical (median ES/BS: placebo 6.3%, romosozumab 1.6%; P = 0.003) bone. At 12 months, cancellous bone formation was significantly lower (P < 0.05 to P < 0.001) in romosozumab versus placebo and the lower values for resorption endpoints seen at month 2 persisted (P < 0.001), signaling a decrease in bone turnover (P = 0.006). No significant change was observed in periosteal and endocortical bone. This resulted in an increase in bone mass and trabecular thickness with improved trabecular connectivity, without significant modification of cortical porosity at month 12. In conclusion, romosozumab produced an early and transient increase in bone formation, but a persistent decrease in bone resorption. Antiresorptive action eventually resulted in decreased bone turnover. This effect resulted in significant increases in bone mass and improved microarchitecture. © 2019 American Society for Bone and Mineral Research.
Trial registration: ClinicalTrials.gov NCT01575834.
Keywords: BONE HISTOMORPHOMETRY; BONE MODELING; BONE REMODELING; MICROCOMPUTED TOMOGRAPHY; OSTEOPOROSIS.
© 2019 American Society for Bone and Mineral Research.
Figures
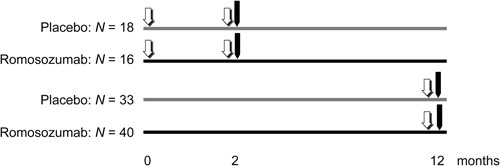
 one set of double fluorochrome labeling,
one set of double fluorochrome labeling,  transiliac bone biopsy)
transiliac bone biopsy)
References
-
- NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis and Therapy. Osteoporosis prevention, diagnosis and therapy. JAMA. 2001;285:785–95. - PubMed
-
- Boivin GY, Chavassieux PM, Santora AC, Yates J, Meunier PJ. Alendronate increases bone strength by increasing the mean degree of mineralization of bone tissue in osteoporotic women. Bone. 2000;27:687–94. - PubMed
-
- Arlot M, Meunier PJ, Boivin G, et al. Differential effects of teriparatide and alendronate on bone remodeling in postmenopausal women assessed by histomorphometric parameters. J Bone Miner Res. 2005;20:1244–53. - PubMed
-
- Poole KE, van Bezooijen RL, Loveridge N, et al. Sclerostin is a delayed secreted product of osteocytes that inhibits bone formation. FASEB J. 2005;19:1842–4. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
