

Cardiovascular Risk Scores to Predict Perioperative Stroke in Noncardiac Surgery
- PMID: 31234757
- PMCID: PMC10027603
- DOI: 10.1161/STROKEAHA.119.024995
Cardiovascular Risk Scores to Predict Perioperative Stroke in Noncardiac Surgery
Abstract
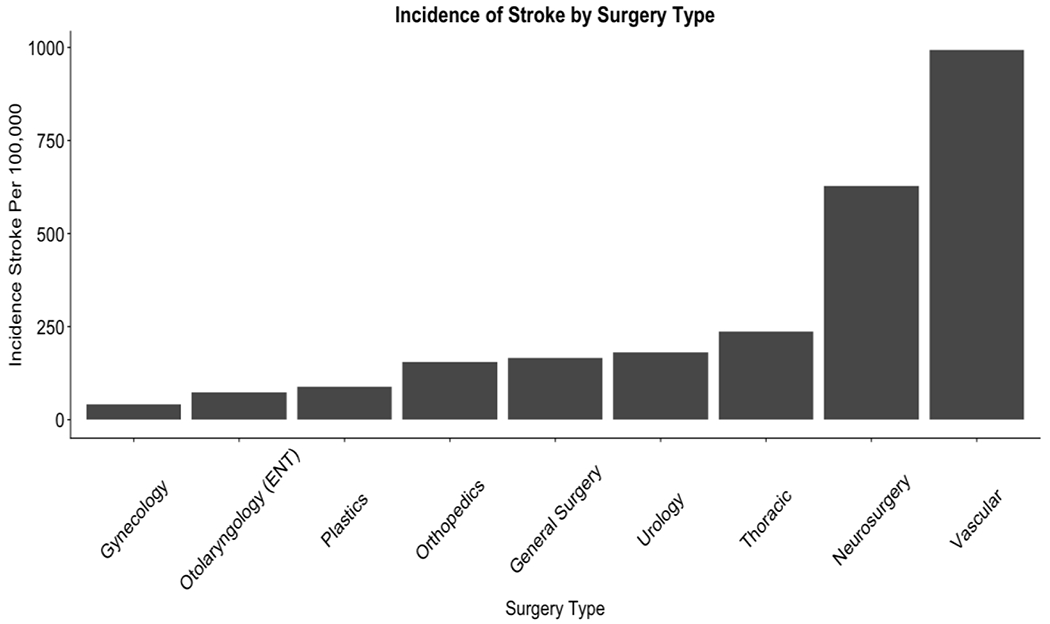
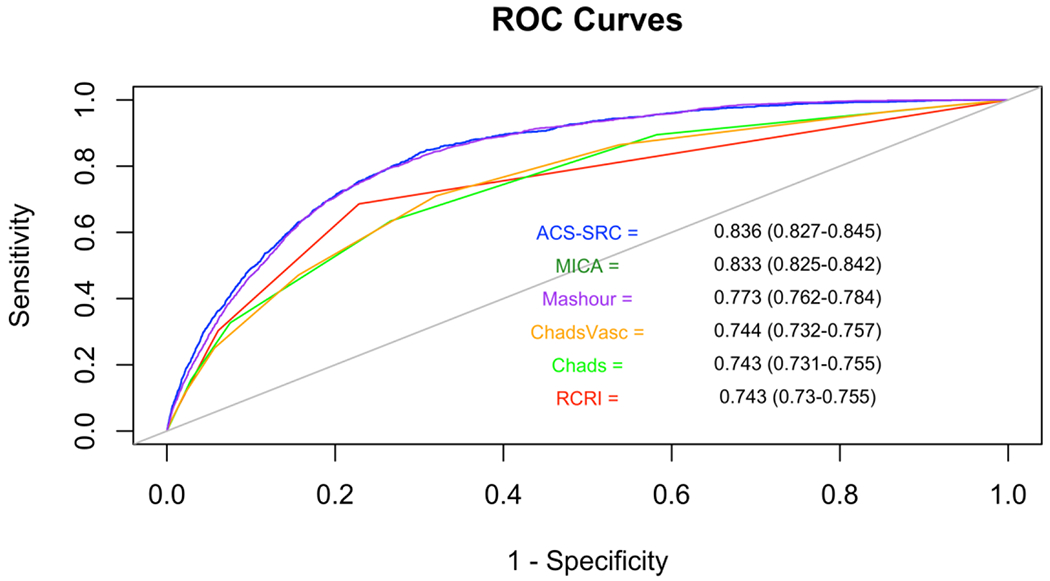
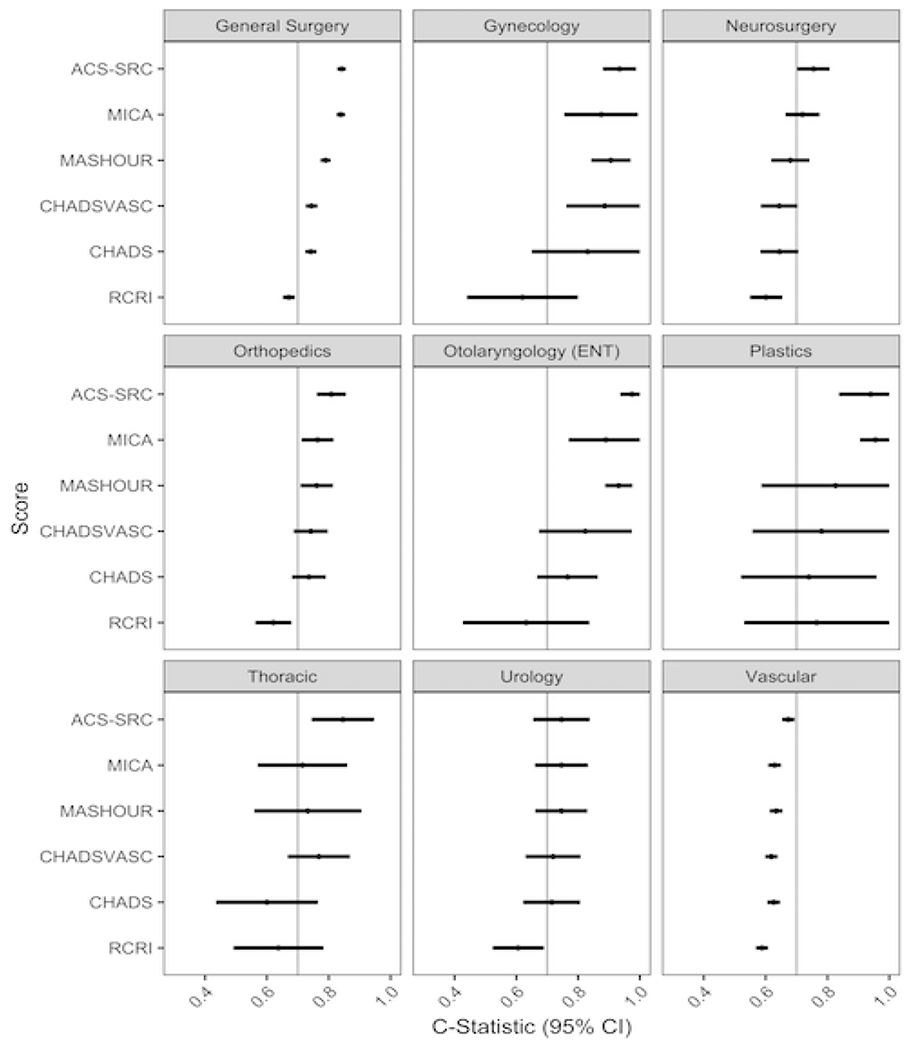
Background and Purpose- Perioperative stroke is associated with significant morbidity and mortality. Conventional cardiovascular risk scores have not been compared to predict acute stroke after noncardiac surgery. Methods- Patients undergoing noncardiac surgery between 2009 and 2010 were identified from the US National Surgical Quality Improvement Program (n=540 717). Patients were prospectively followed for 30 days postoperatively for the primary outcome of stroke. Established cardiovascular and perioperative risk scores (CHADS2, CHA2DS2-VASc, Revised Cardiac Risk Index, Mashour et al risk score, Myocardial Infarction or Cardiac Arrest risk score, and National Quality Improvement Project American College of Surgeons surgical risk calculator) were assessed to predict perioperative stroke. Results- Stroke occurred in the perioperative period of 1474 noncardiac surgeries (0.27%). Patients with perioperative stroke were older, more frequently male, had lower body mass index, and were more likely to have undergone vascular surgery or neurosurgery than patients without stroke (P<0.001 for each comparison). All risk prediction models were associated with increased risk of perioperative stroke (C statistic [AUC] range, 0.743-0.836). The Myocardial Infarction or Cardiac Arrest risk score (AUC, 0.833) and American College of Surgeons surgical risk calculator (AUC, 0.836) had the most favorable test characteristics and a greater ability to discriminate perioperative stroke when compared with Revised Cardiac Risk Index, CHADS2, CHA2DS2-VASc, and Mashour risk scores (P for comparison, <0.001; Delong). Risk scores did not provide consistent discriminative ability across surgery types and were least predictive in vascular surgery (AUC range, 0.588-0.672). Conclusions- The Myocardial Infarction or Cardiac Arrest risk score and American College of Surgeons surgical risk calculator surgical risk scores provide excellent risk discrimination for perioperative stroke in most patients undergoing noncardiac surgery. Stroke prediction was less optimal in patients undergoing vascular surgery.
Keywords: forecasting; humans; male; preoperative care; stroke.
Conflict of interest statement
Conflict of Interest Disclosures: None.
Figures
Similar articles
-
Development and Validation of a Prediction Model for Stroke, Cardiac, and Mortality Risk After Non-Cardiac Surgery.J Am Heart Assoc. 2021 Feb 16;10(4):e018013. doi: 10.1161/JAHA.120.018013. Epub 2021 Jan 30. J Am Heart Assoc. 2021. PMID: 33522252 Free PMC article.
-
Combining CHA2DS2-VASc score into RCRI for prediction perioperative cardiovascular outcomes in patients undergoing non-cardiac surgery: a retrospective pilot study.BMC Anesthesiol. 2021 Nov 9;21(1):276. doi: 10.1186/s12871-021-01496-2. BMC Anesthesiol. 2021. PMID: 34753422 Free PMC article.
-
Which risk score best predicts perioperative outcomes in nonvalvular atrial fibrillation patients undergoing noncardiac surgery?Am Heart J. 2014 Jul;168(1):60-7.e5. doi: 10.1016/j.ahj.2014.03.015. Epub 2014 Apr 3. Am Heart J. 2014. PMID: 24952861
-
Perioperative Cardiovascular Risk Assessment and Management for Noncardiac Surgery: A Review.JAMA. 2020 Jul 21;324(3):279-290. doi: 10.1001/jama.2020.7840. JAMA. 2020. PMID: 32692391 Review.
-
Preoperative cardiovascular evaluation for noncardiac surgery.Mt Sinai J Med. 2005 May;72(3):185-92. Mt Sinai J Med. 2005. PMID: 15915313 Review.
Cited by
-
Perioperative stroke.Nat Rev Dis Primers. 2024 Jan 18;10(1):3. doi: 10.1038/s41572-023-00487-6. Nat Rev Dis Primers. 2024. PMID: 38238382 Review.
-
Development and Validation of a Prediction Model for Stroke, Cardiac, and Mortality Risk After Non-Cardiac Surgery.J Am Heart Assoc. 2021 Feb 16;10(4):e018013. doi: 10.1161/JAHA.120.018013. Epub 2021 Jan 30. J Am Heart Assoc. 2021. PMID: 33522252 Free PMC article.
-
Prediction for Perioperative Stroke Using Intraoperative Parameters.J Am Heart Assoc. 2024 Aug 20;13(16):e032216. doi: 10.1161/JAHA.123.032216. Epub 2024 Aug 9. J Am Heart Assoc. 2024. PMID: 39119968 Free PMC article.
-
Risk factor analysis and creation of an externally-validated prediction model for perioperative stroke following non-cardiac surgery: A multi-center retrospective and modeling study.PLoS Med. 2025 Mar 21;22(3):e1004539. doi: 10.1371/journal.pmed.1004539. eCollection 2025 Mar. PLoS Med. 2025. PMID: 40117288 Free PMC article.
-
Timing of Postoperative Stroke and Risk of Mortality After Noncardiac Surgery: A Cohort Study.J Clin Med Res. 2023 May;15(5):268-273. doi: 10.14740/jocmr4877. Epub 2023 May 31. J Clin Med Res. 2023. PMID: 37303467 Free PMC article.
References
-
- Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130:2215–2245. - PubMed
-
- Gupta PK, Gupta H, Sundaram A, Kaushik M, Fang X, Miller WJ, et al. Development and validation of a risk calculator for prediction of cardiac risk after surgery. Circulation. 2011;124:381–387. - PubMed
-
- Bilimoria KY, Liu Y, Paruch JL, Zhou L, Kmiecik TE, Ko CY, et al. Development and evaluation of the universal ACS NSQIP surgical risk calculator: a decision aid and informed consent tool for patients and surgeons. Journal of the American College of Surgeons. 2013;217:833–842.e831-833. - PMC - PubMed
-
- Peguero JG, Issa O, Podesta C, Elmahdy HM, Santana O, Lamas GA. Usefulness of the CHA2DS2VASc score to predict postoperative stroke in patients having cardiac surgery independent of atrial fibrillation. The American journal of cardiology. 2015;115:758–762. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
