

A long-term follow-up study on otoacoustic emissions testing in paediatric patients with severe malaria in Gabon
- PMID: 31234890
- PMCID: PMC6591898
- DOI: 10.1186/s12936-019-2840-9
A long-term follow-up study on otoacoustic emissions testing in paediatric patients with severe malaria in Gabon
Abstract
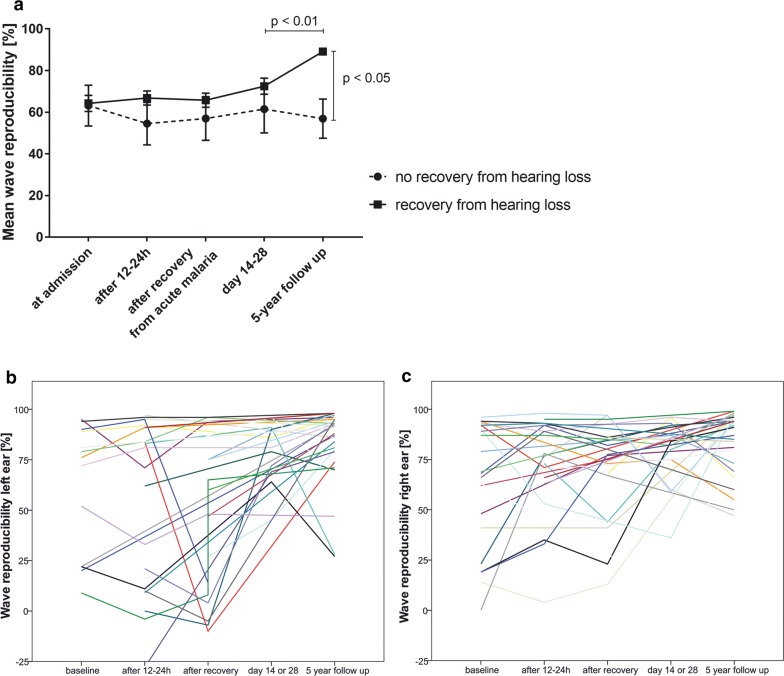
Background: In a previous study, severe and cerebral malaria have been connected with acute cochlear malfunction in children, demonstrated by a decrease of transitory evoked otoacoustic emissions (TEOAEs) reproducibility. This study aims to determine whether cochlear malfunction persists for 4 years after recovery from severe malaria in a subset of the previous study's collective. Follow-up TEOAEs were performed on site (CERMEL, Hôpital Albert Schweitzer, Lambaréné, Gabon) or at the participants' homes; 33 out of 90 participants included in the initial investigation by Schmutzhard et al. could be retrieved and were re-examined, 31/33 could be included. Of the 57 missing participants, 51 could not be contacted, 1 had moved away, 4 refused to cooperate, and 1 had died.
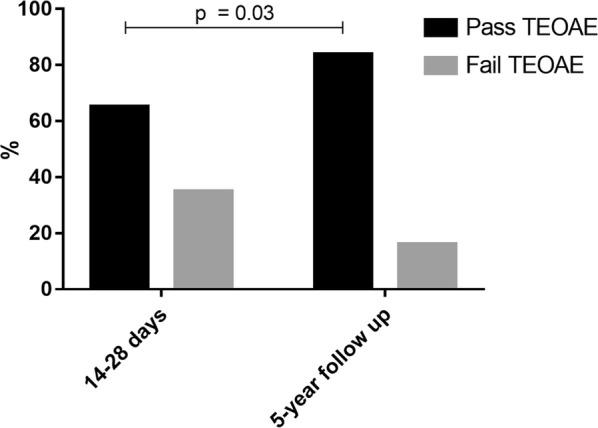
Methods: As in the initial investigation, participants of this prospective follow-up study were subjected to TEOAE examination on both ears separately. A wave correlation rate of > 60% on both ears was considered a "pass"; if one ear failed to pass, the examination was considered a "fail". The results were compared to the primary control group. Additionally, a questionnaire has been applied focusing on subsequent malaria infections between the primary inclusion and follow-up and subjective impairment of hearing and/or understanding.
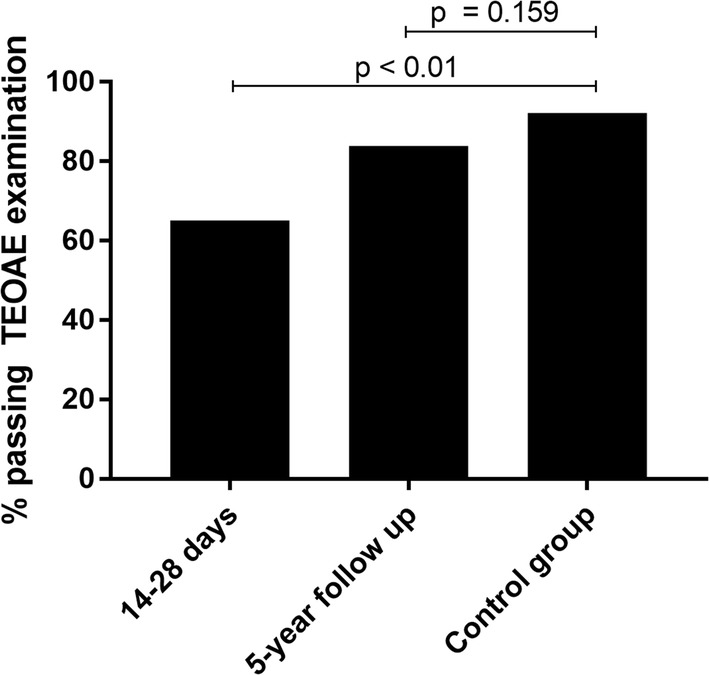
Results: The cohort's mean age was 9 years, 14 children were female, 18 male. 31 had been originally admitted with severe, one with cerebral malaria. 83.8% of participants (n = 26) presented with a TEOAE correlation rate of > 60% on both ears (the cut-off for good cochlear function); in the control group, 92.2% (n = 83) had passed TEOAE examination on both ears. Recurrent severe malaria was associated with a worse TEOAE correlation rate. Age at infection and gender had no influence on the outcome.
Conclusions: Cochlear malfunction seems to be persistent after 4 years in more than 16% of children hospitalized for malaria. In a healthy control group, this proportion was 7.8%. Yet, the severity of the initial TEOAE-decrease did not predict a worse outcome.
Keywords: Children; Hearing loss; Otoacoustic emissions; Severe malaria.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Severe malaria in children leads to a significant impairment of transitory otoacoustic emissions--a prospective multicenter cohort study.BMC Med. 2015 May 28;13:125. doi: 10.1186/s12916-015-0366-8. BMC Med. 2015. PMID: 26021376 Free PMC article.
-
A role for otoacoustic emissions in screening for hearing impairment and middle ear disorders in school-age children.Ear Hear. 1997 Jun;18(3):227-39. doi: 10.1097/00003446-199706000-00006. Ear Hear. 1997. PMID: 9201458
-
Transient-evoked otoacoustic emissions in a group of professional singers who have normal pure-tone hearing thresholds.Ear Hear. 2008 Jun;29(3):360-77. doi: 10.1097/AUD.0b013e31816a0d1e. Ear Hear. 2008. PMID: 18382377
-
A review of the effectiveness of otoacoustic emissions for evaluating hearing status after newborn screening.Otol Neurotol. 2013 Aug;34(6):1058-63. doi: 10.1097/MAO.0b013e318282964f. Otol Neurotol. 2013. PMID: 23628790 Review.
-
Otoacoustic emissions: a new method to diagnose hearing impairment in children.Eur J Pediatr. 1993 Aug;152(8):626-34. doi: 10.1007/BF01955236. Eur J Pediatr. 1993. PMID: 8404964 Review.
Cited by
-
The Ototoxicity of Antimalarial Drugs-A State of the Art Review.Front Neurol. 2021 Apr 20;12:661740. doi: 10.3389/fneur.2021.661740. eCollection 2021. Front Neurol. 2021. PMID: 33959089 Free PMC article. Review.
-
Hearing thresholds elevation and potential association with emotional problems among 1,914 children in Beijing, China.Front Public Health. 2022 Aug 4;10:937301. doi: 10.3389/fpubh.2022.937301. eCollection 2022. Front Public Health. 2022. PMID: 35991012 Free PMC article.
References
-
- Fusetti M, Eibenstein A, Corridore V, Hueck S, Chiti-Batelli S. Mefloquine and ototoxicity: a report of 3 cases. Clin Ter. 1999;150:379–382. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
