

Gait Abnormalities and the Risk of Falls in CKD
- PMID: 31235462
- PMCID: PMC6625617
- DOI: 10.2215/CJN.13871118
Gait Abnormalities and the Risk of Falls in CKD
Abstract
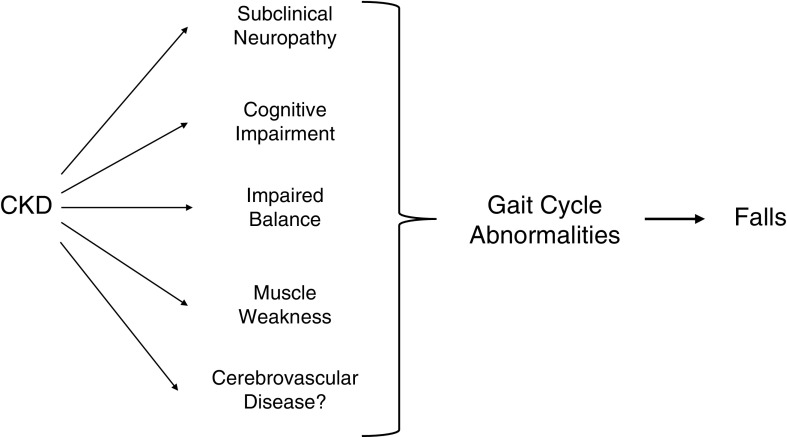
Background and objectives: Older adults with CKD are at high risk of falls and disability. It is not known whether gait abnormalities contribute to this risk.
Design, setting, participants, & measurements: Quantitative and clinical gait assessments were performed in 330 nondisabled community-dwelling adults aged ≥65 years. CKD was defined as an eGFR <60 ml/min per 1.73 m2. Cox proportional hazards models were created to examine fall risk.
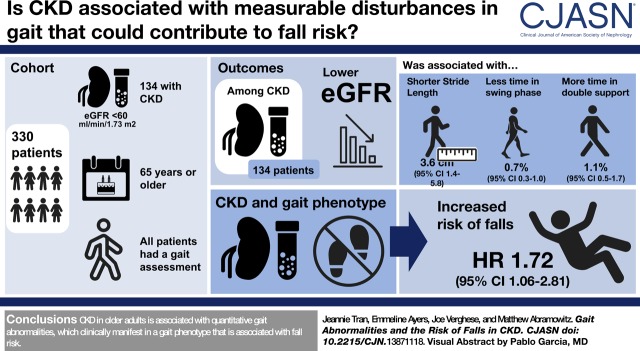
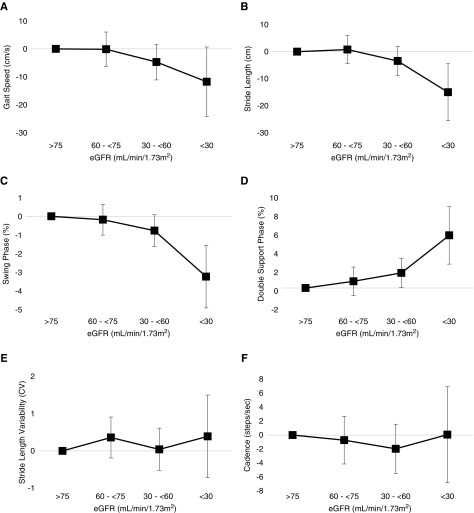
Results: A total of 41% (n=134) of participants had CKD. In addition to slower gait speed, participants with CKD had gait cycle abnormalities including shorter stride length and greater time in the stance and double-support phases. Among people with CKD, lower eGFR was independently associated with the severity of gait cycle abnormalities (per 10 ml/min per 1.73 m2 lower eGFR: 3.6 cm [95% confidence interval (95% CI), 1.4 to 5.8] shorter stride length; 0.7% [95% CI, 0.3 to 1.0] less time in swing phase; 1.1% [95% CI, 0.5 to 1.7] greater time in double-support phase); these abnormalities mediated the association of lower eGFR with slower gait speed. On clinical gait exam, consistent with the quantitative abnormalities, short steps and marked swaying or loss of balance were more common among participants with CKD, yet most had no identifiable gait phenotype. A gait phenotype defined by any of these abnormal signs was associated with higher risk of falls among participants with CKD: compared with people without CKD and without the gait phenotype, the adjusted hazard ratio was 1.72 (95% CI, 1.06 to 2.81) for those with CKD and the phenotype; in comparison, the adjusted hazard ratio was 0.71 (95% CI, 0.40 to 1.25) for people with CKD but without the phenotype (P value for interaction of CKD status and gait phenotype =0.01).
Conclusions: CKD in older adults is associated with quantitative gait abnormalities, which clinically manifest in a gait phenotype that is associated with fall risk.
Keywords: Accidental Falls; Gait; Independent Living; Phenotype; Proportional Hazards Models; Receptor, Epidermal Growth Factor; Renal Insufficiency, Chronic; Risk; Walking Speed; chronic kidney disease; eGFR protein, human; geriatric nephrology; glomerular filtration rate.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
-
Targeting Fall Risk in CKD.Clin J Am Soc Nephrol. 2019 Jul 5;14(7):965-966. doi: 10.2215/CJN.06040519. Epub 2019 Jun 24. Clin J Am Soc Nephrol. 2019. PMID: 31278111 Free PMC article. No abstract available.
References
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, van Lente F, Levey AS: Prevalence of chronic kidney disease in the United States. JAMA 298: 2038–2047, 2007 - PubMed
-
- Murphy D, McCulloch CE, Lin F, Banerjee T, Bragg-Gresham JL, Eberhardt MS, Morgenstern H, Pavkov ME, Saran R, Powe NR, Hsu CY; Centers for Disease Control and Prevention Chronic Kidney Disease Surveillance Team : Trends in prevalence of chronic kidney disease in the United States. Ann Intern Med 165: 473–481, 2016 - PMC - PubMed
-
- Fried LF, Lee JS, Shlipak M, Chertow GM, Green C, Ding J, Harris T, Newman AB: Chronic kidney disease and functional limitation in older people: Health, aging and body composition study. J Am Geriatr Soc 54: 750–756, 2006 - PubMed
-
- Cook WL, Tomlinson G, Donaldson M, Markowitz SN, Naglie G, Sobolev B, Jassal SV: Falls and fall-related injuries in older dialysis patients. Clin J Am Soc Nephrol 1: 1197–1204, 2006 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
