

Feasibility of combined screening for upper gastrointestinal adenocarcinoma risk by serology and Cytosponge testing: the SUGAR study
- PMID: 31235543
- PMCID: PMC6874497
- DOI: 10.1136/jclinpath-2019-205700
Feasibility of combined screening for upper gastrointestinal adenocarcinoma risk by serology and Cytosponge testing: the SUGAR study
Abstract
Aims: Aim was to assess the feasibility of serum markers to identify individuals at risk for gastro-oesophageal adenocarcinoma to reduce the number of individuals requiring invasive assessment by endoscopy.
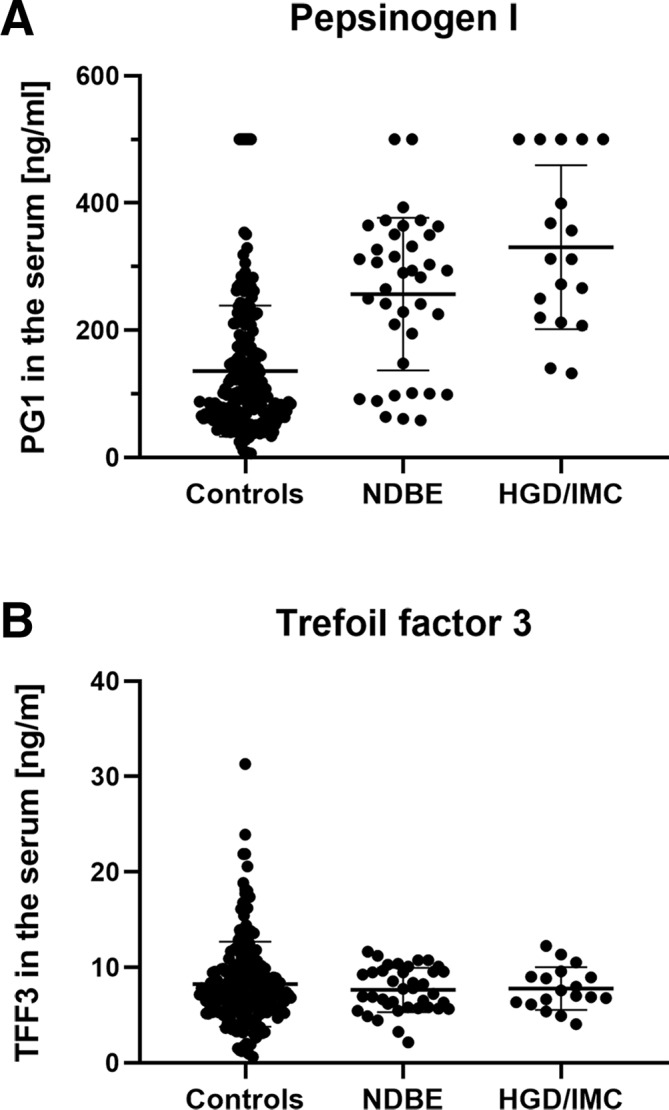
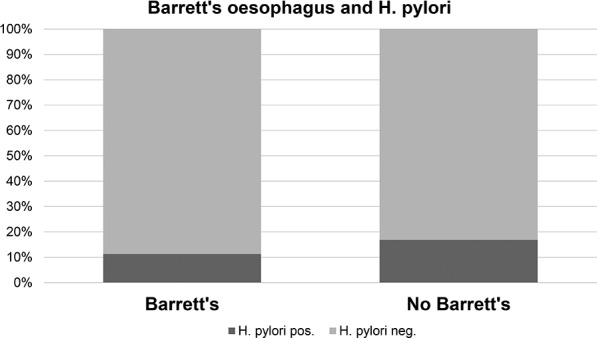
Methods: Blood samples from 56 patients with Barrett's oesophagus and 202 non-Barrett controls who previously took part in a trial assessing the accuracy of the Cytosponge for Barrett's oesophagus were assessed for serum pepsinogen (PG) 1 and 2, gastrin-17, trefoil factor 3 (TFF3) and Helicobacter pylori infection.
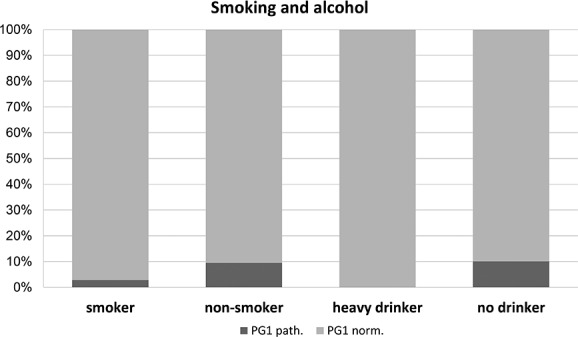
Results: PG1 was pathological (<50 ng/mL) in 26 patients (10.1%), none of whom had Barrett's oesophagus (p<0.001). Smoking and drinking had no influence on these results. Pathological PG1 was associated with stomach pain (p=0.029), disruption of sleep (p=0.027) and disruption of diet by symptoms (p=0.019). Serum TFF3 was not associated with any clinical parameter.
Conclusions: Assessment of serum PG1 could be combined with a test for Barrett's oesophagus to identify additional patients requiring endoscopy.
Keywords: TFF3; barrett’s oesophagus; gastric atrophy; gastric cancer; pepsinogens.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Dinis-Ribeiro M, Areia M, de Vries AC, et al. . Management of precancerous conditions and lesions in the stomach (MAPs): guideline from the European Society of gastrointestinal endoscopy (ESGE), European Helicobacter Study Group (EHSG), European Society of pathology (esp), and the Sociedade Portuguesa de Endoscopia Digestiva (SPED). Endoscopy 2012;44:74–94. 10.1055/s-0031-1291491 - DOI - PMC - PubMed
-
- Roman LD, Lukyanchuk R, Sablin OA, et al. . Prevalence of H. pylori infection and atrophic gastritis in a population-based screening with serum biomarker panel (GastroPanel®) in St. Petersburg. Anticancer Res 2016;36:4129–38. - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical