

Anti-hepatitis C virus therapy in chronic kidney disease patients improves long-term renal and patient survivals
- PMID: 31236391
- PMCID: PMC6580345
- DOI: 10.12998/wjcc.v7.i11.1270
Anti-hepatitis C virus therapy in chronic kidney disease patients improves long-term renal and patient survivals
Abstract
Background: Hepatitis C virus (HCV) infection is a documented risk factor for chronic kidney disease (CKD) and progression to end-stage renal disease (ESRD). However, to date there are no reports on the long-term hard endpoints (ESRD and death) of anti-HCV therapy [interferon-based therapy (IBT) or new direct-acting antivirals] in CKD patients. Direct-acting antivirals are not available in Taiwan's single-payer national health insurance database currently released for research. Therefore, we hypothesized that a retrospective analysis of the long-term outcomes of IBT in CKD patients will serve as a proxy for direct-acting antivirals to increase our understanding of progression to ESRD following HCV infection.
Aim: To evaluate the long-term outcomes (ESRD and death) of anti-HCV therapy, especially IBT, in HCV-infected patients with stage 1-5 CKD.
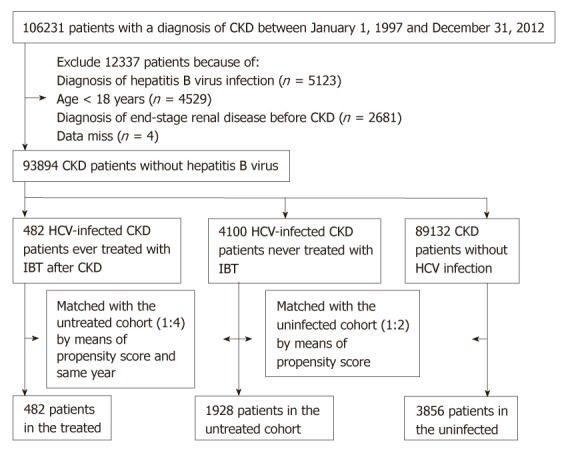
Methods: We analyzed 93894 Taiwanese adults diagnosed with CKD and without HBV infection. Of these, 4.9% were infected with HCV. Of the 4582 HCV-infected CKD patients, 482 (10.5%) received IBT (treated cohort). They were matched 1:4 with 1928 untreated HCV-infected CKD patients (untreated cohort) by propensity scores and year, which further matched 1:2 by propensity scores with 3856 CKD patients without HCV infection (uninfected cohort). All participants were followed until the occurrence of ESRD, death, or the end of 2012. The association between HCV infection, IBT use, and risks of ESRD and death was analyzed using competing risk analysis.
Results: Taking the uninfected cohort as a reference, the adjusted hazard ratios for ESRD, after adjusting for competing mortality, were 0.34 (0.14-0.84, P = 0.019) and 1.28 (1.03-1.60, P = 0.029) in the treated and untreated cohorts, respectively. The treated cohort had a 29% (0.54-0.92, P = 0.011) decrease in mortality compared to the untreated cohort, in which the mortality was 31% (1.18-1.45, P < 0.001) higher than in the uninfected cohort. The reduced risks of ESRD (0.14, 0.03-0.58, P = 0.007) and death (0.57, 0.41-0.79, P = 0.001) were greatest in HCV-infected CKD patients who received at least 4 mo of IBT, which accounted for 74% of the treated cohort.
Conclusion: Adequate anti-HCV therapy in CKD patients improves long-term renal and patient survival.
Keywords: Anti-hepatitis C virus therapy; Chronic kidney disease; Cohort study; End-stage renal disease; Hepatitis C virus.
Conflict of interest statement
Conflict-of-interest statement: All authors have no conflict of interests.
Figures
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) KDIGO clinical practice guidelines for the prevention, diagnosis, evaluation, and treatment of hepatitis C in chronic kidney disease. Kidney Int Suppl. 2008;109:S1–99. - PubMed
-
- Chacko EC, Surrun SK, Mubarack Sani TP, Pappachan JM. Chronic viral hepatitis and chronic kidney disease. Postgrad Med J. 2010;86:486–492. - PubMed
-
- Perico N, Cattaneo D, Bikbov B, Remuzzi G. Hepatitis C infection and chronic renal diseases. Clin J Am Soc Nephrol. 2009;4:207–220. - PubMed
-
- Chen YC, Lin HY, Li CY, Lee MS, Su YC. A nationwide cohort study suggests that hepatitis C virus infection is associated with increased risk of chronic kidney disease. Kidney Int. 2014;85:1200–1207. - PubMed
LinkOut - more resources
Full Text Sources
