

Expiratory muscle dysfunction in critically ill patients: towards improved understanding
- PMID: 31236639
- PMCID: PMC6667683
- DOI: 10.1007/s00134-019-05664-4
Expiratory muscle dysfunction in critically ill patients: towards improved understanding
Abstract
Introduction: This narrative review summarizes current knowledge on the physiology and pathophysiology of expiratory muscle function in ICU patients, as shared by academic professionals from multidisciplinary, multinational backgrounds, who include clinicians, clinical physiologists and basic physiologists.
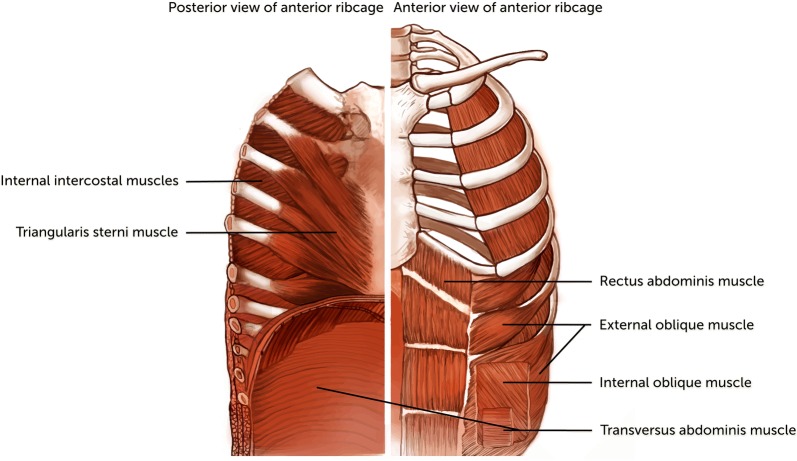
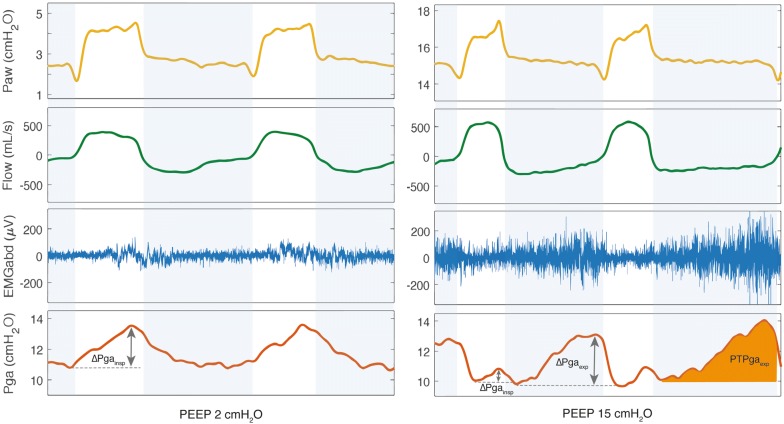
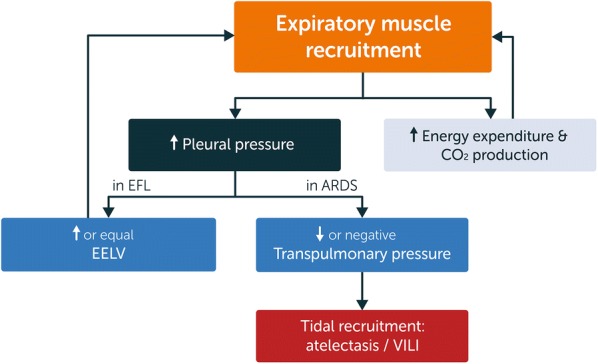
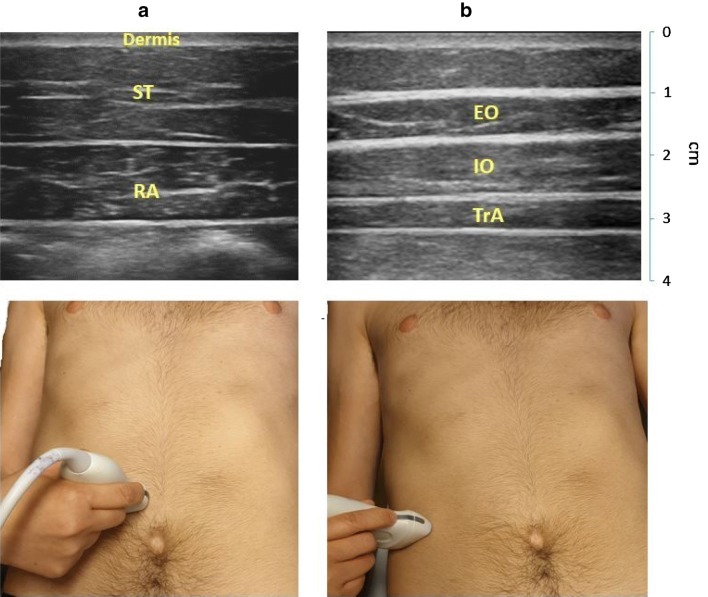
Results: The expiratory muscles, which include the abdominal wall muscles and some of the rib cage muscles, are an important component of the respiratory muscle pump and are recruited in the presence of high respiratory load or low inspiratory muscle capacity. Recruitment of the expiratory muscles may have beneficial effects, including reduction in end-expiratory lung volume, reduction in transpulmonary pressure and increased inspiratory muscle capacity. However, severe weakness of the expiratory muscles may develop in ICU patients and is associated with worse outcomes, including difficult ventilator weaning and impaired airway clearance. Several techniques are available to assess expiratory muscle function in the critically ill patient, including gastric pressure and ultrasound.
Conclusion: The expiratory muscles are the "neglected component" of the respiratory muscle pump. Expiratory muscles are frequently recruited in critically ill ventilated patients, but a fundamental understanding of expiratory muscle function is still lacking in these patients.
Keywords: Acute respiratory failure; Expiratory muscles; Mechanical ventilation; Respiratory muscle monitoring; Respiratory muscle weakness.
Figures


References
-
- De Troyer A, Boriek AM. Mechanics of the respiratory muscles. Compr Physiol. 2011;1:1273–1300. - PubMed
-
- Goligher EC, Fan E, Herridge MS, Murray A, Vorona S, Brace D, Rittayamai N, Lanys A, Tomlinson G, Singh JM, Bolz SS, Rubenfeld GD, Kavanagh BP, Brochard LJ, Ferguson ND. Evolution of diaphragm thickness during mechanical ventilation. impact of inspiratory effort. Am J Respir Crit Care Med. 2015;192:1080–1088. doi: 10.1164/rccm.201503-0620OC. - DOI - PubMed
-
- Jaber S, Petrof BJ, Jung B, Chanques G, Berthet JP, Rabuel C, Bouyabrine H, Courouble P, Koechlin-Ramonatxo C, Sebbane M, Similowski T, Scheuermann V, Mebazaa A, Capdevila X, Mornet D, Mercier J, Lacampagne A, Philips A, Matecki S. Rapidly progressive diaphragmatic weakness and injury during mechanical ventilation in humans. Am J Respir Crit Care Med. 2011;183:364–371. doi: 10.1164/rccm.201004-0670OC. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
