

Septal total atrial conduction time for prediction of atrial fibrillation in embolic stroke of unknown source: a pilot study
- PMID: 31236691
- PMCID: PMC6989646
- DOI: 10.1007/s00392-019-01501-2
Septal total atrial conduction time for prediction of atrial fibrillation in embolic stroke of unknown source: a pilot study
Abstract
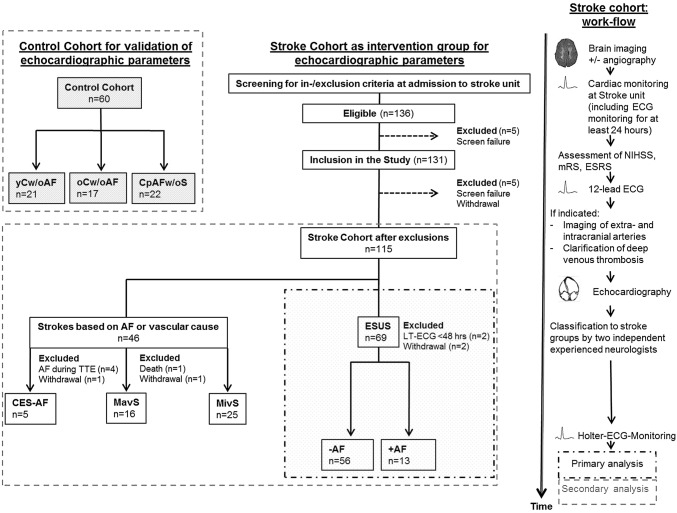
Background: Subclinical atrial fibrillation (AF) is the underlying cause in a relevant part of patients with embolic stroke of unknown source (ESUS). This pilot study aims to identify novel echocardiographic parameters predicting AF subsequently detected in patients originally hospitalized with ESUS.
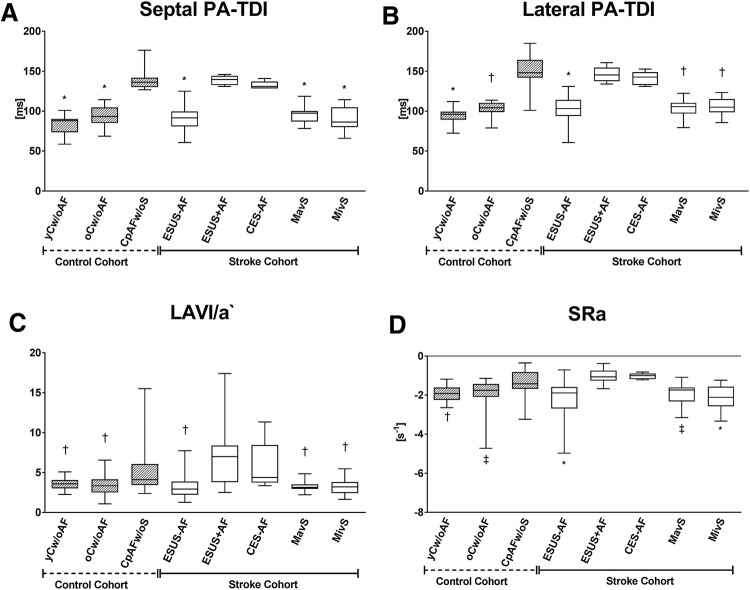
Methods and results: Patients with acute ischemic stroke [baseline diagnosis of ESUS (n = 69), stroke of macro- or microvascular cause (n = 16/25), stroke caused by AF (n = 5)] and controls with paroxysmal AF without acute ischemic stroke (n = 22) as well as healthy controls of young and old age (n = 21/17) in sinus rhythm were included (overall n = 175). Echocardiography was performed in all participants. Prolonged Holter-ECG-monitoring was performed in all stroke patients. In the overall cohort, septal total atrial conduction time (sPA-TDI), left atrial (LA) volume index to tissue Doppler velocity (LAVI/a`) and second negative peak strain rate during LA contraction (SRa), representing echocardiographic parameters of LA remodelling and function, were statistically significant different in patients with and without AF and predictive for subclinical AF (multivariate regression analysis: sPA-TDI: HR 1.06 [1.04-1.08], p < 0.001; LAVI/a`: HR 0.85, [0.74-0.97], p = 0.02; SRa: HR 2.35 [0.9-5.5], p = 0.05). Multivariate Cox regression analysis revealed sPA-TDI as an independent predictor of AF in ESUS patients (sPA-TDI: HR 1.10 [1.04-1.17], p = 0.001). A sPA-TDI of 126 ms strictly discriminated between presence and absence of subclinical AF within 48 h after initiation of Holter-ECG-monitoring in ESUS patients.
Conclusions: sPA-TDI seems to be a strong independent predictor of subclinical AF in patients hospitalized for ESUS and might support risk-stratified clinical decision making in these patients. Septal Total Atrial Conduction Time (sPA-TDI) determined by echocardiography for prediction of Atrial Fibrillation in Embolic Stroke of Unknown Source (ESUS).
Keywords: Atrial fibrillation; ESUS; Echocardiography; Stroke.
Conflict of interest statement
All authors have no conflict of interest to declare.
Figures

Similar articles
-
A Simple Score That Predicts Paroxysmal Atrial Fibrillation on Outpatient Cardiac Monitoring after Embolic Stroke of Unknown Source.J Stroke Cerebrovasc Dis. 2018 Jun;27(6):1692-1696. doi: 10.1016/j.jstrokecerebrovasdis.2018.01.028. Epub 2018 Feb 28. J Stroke Cerebrovasc Dis. 2018. PMID: 29501269
-
Transient atrial mechanical dysfunction assessed in acute phase of embolic stroke of undetermined source.J Stroke Cerebrovasc Dis. 2020 Sep;29(9):105032. doi: 10.1016/j.jstrokecerebrovasdis.2020.105032. Epub 2020 Jun 23. J Stroke Cerebrovasc Dis. 2020. PMID: 32807444
-
Artificial Intelligence-Enabled ECG to Identify Silent Atrial Fibrillation in Embolic Stroke of Unknown Source.J Stroke Cerebrovasc Dis. 2021 Sep;30(9):105998. doi: 10.1016/j.jstrokecerebrovasdis.2021.105998. Epub 2021 Jul 22. J Stroke Cerebrovasc Dis. 2021. PMID: 34303963
-
Detection and management of atrial fibrillation after cryptogenic stroke or embolic stroke of undetermined source.Clin Cardiol. 2018 Mar;41(3):426-432. doi: 10.1002/clc.22876. Epub 2018 Mar 22. Clin Cardiol. 2018. PMID: 29569253 Free PMC article. Review.
-
Detection of Atrial Fibrillation in Cryptogenic Stroke.Curr Neurol Neurosci Rep. 2018 Aug 8;18(10):66. doi: 10.1007/s11910-018-0871-1. Curr Neurol Neurosci Rep. 2018. PMID: 30090997 Review.
Cited by
-
Left Ventricular Diastolic Dysfunction with Elevated Filling Pressures Is Associated with Embolic Stroke of Undetermined Source and Atrial Fibrillation.Tomography. 2024 Oct 14;10(10):1694-1705. doi: 10.3390/tomography10100124. Tomography. 2024. PMID: 39453041 Free PMC article.
-
The Role of Galectin-3 Levels for Predicting Paroxysmal Atrial Fibrillation in Patients with Embolic Stroke of Undetermined Source.J Clin Med. 2024 May 29;13(11):3175. doi: 10.3390/jcm13113175. J Clin Med. 2024. PMID: 38892886 Free PMC article.
-
Cardiac function and atrial conduction time in morbid obesity: Insights from an echocardiographic case-control study.Glob Cardiol Sci Pract. 2025 Feb 28;2025(1):e202513. doi: 10.21542/gcsp.2025.13. eCollection 2025 Feb 28. Glob Cardiol Sci Pract. 2025. PMID: 40390991 Free PMC article.
-
Atrial strain and occult atrial fibrillation in cryptogenic stroke patients: a systematic review and meta-analysis.Clin Res Cardiol. 2023 Nov;112(11):1600-1609. doi: 10.1007/s00392-023-02218-z. Epub 2023 May 8. Clin Res Cardiol. 2023. PMID: 37154833
-
Circulating fibroblast activation protein α is reduced in acute ischemic stroke.Front Cardiovasc Med. 2022 Dec 7;9:1064157. doi: 10.3389/fcvm.2022.1064157. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36568546 Free PMC article.
References
-
- Hart RG, Diener HC, Coutts SB, Easton JD, Granger CB, O’Donnell MJ, Sacco RL, Connolly SJ, Cryptogenic Stroke/ESUS International Working Group Embolic strokes of undetermined source: the case for a new clinical construct. Lancet Neurol. 2014;13:429–438. doi: 10.1016/S1474-4422(13)70310-7. - DOI - PubMed
-
- Gladstone DJ, Spring M, Dorian P, Panzov V, Thorpe KE, Hall J, Vaid H, O’Donnell M, Laupacis A, Cote R, Sharma M, Blakely JA, Shuaib A, Hachinski V, Coutts SB, Sahlas DJ, Teal P, Yip S, Spence JD, Buck B, Verreault S, Casaubon LK, Penn A, Selchen D, Jin A, Howse D, Mehdiratta M, Boyle K, Aviv R, Kapral MK, Mamdani M, EMBRACE Investigators and Coordinators Atrial fibrillation in patients with cryptogenic stroke. N Engl J Med. 2014;370:2467–2477. doi: 10.1056/NEJMoa1311376. - DOI - PubMed
-
- Wachter R, Groschel K, Gelbrich G, Hamann GF, Kermer P, Liman J, Seegers J, Wasser K, Schulte A, Jurries F, Messerschmid A, Behnke N, Groschel S, Uphaus T, Grings A, Ibis T, Klimpe S, Wagner-Heck M, Arnold M, Protsenko E, Heuschmann PU, Conen D, Weber-Kruger M, Find-AF(randomised) Investigators and Coordinators Holter-electrocardiogram-monitoring in patients with acute ischaemic stroke (Find-AFRANDOMISED): an open-label randomised controlled trial. Lancet Neurol. 2017;16:282–290. doi: 10.1016/S1474-4422(17)30002-9. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
