

Laparoscopic Approach to Inguinal Disruption in Athletes: a Retrospective 13-Year Analysis of 198 Patients in a Single-Surgeon Setting
- PMID: 31236737
- PMCID: PMC6591337
- DOI: 10.1186/s40798-019-0201-4
Laparoscopic Approach to Inguinal Disruption in Athletes: a Retrospective 13-Year Analysis of 198 Patients in a Single-Surgeon Setting
Abstract
Background: Inguinal disruption (ID) is a condition of chronic groin pain affecting mainly athletes. ID cannot be defined as a true hernia. Pathogenesis is multifactorial due to repetitive and excessive forces applied to the inguino-pelvic region. Examination reveals tenderness to palpation of the inguinal region. Differential diagnosis is challenging; imaging is helpful for excluding other pathologies. Surgery is the treatment of choice when conservative treatment fails. Primary aim of the study was to evaluate the time to return to full sport activity after transabdominal preperitoneal patch plasty (TAPP) technique in ID. Secondary aim was to evaluate the postoperative complication rate both in the immediate post-operative time and in 1 year follow-up and to verify the relapse rate after surgery. In this study, we consider time to return to full sport activity as the time needed to return to pre-injury sport activity.
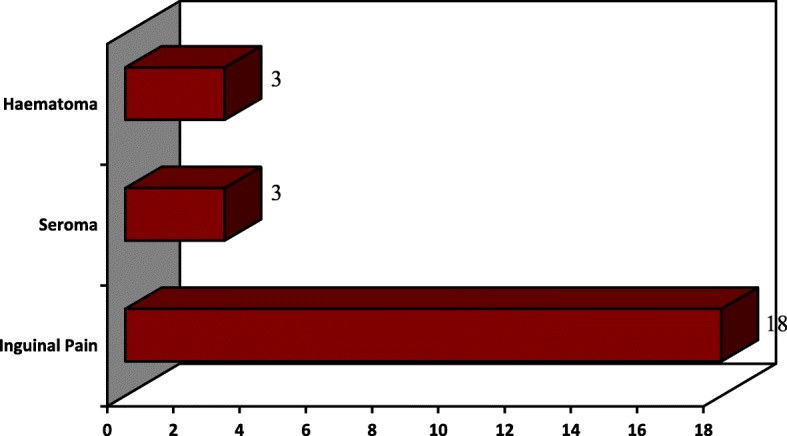
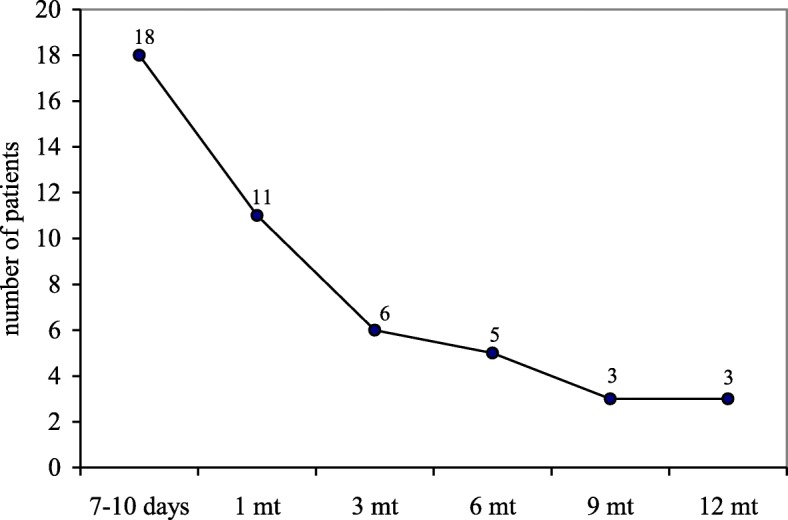
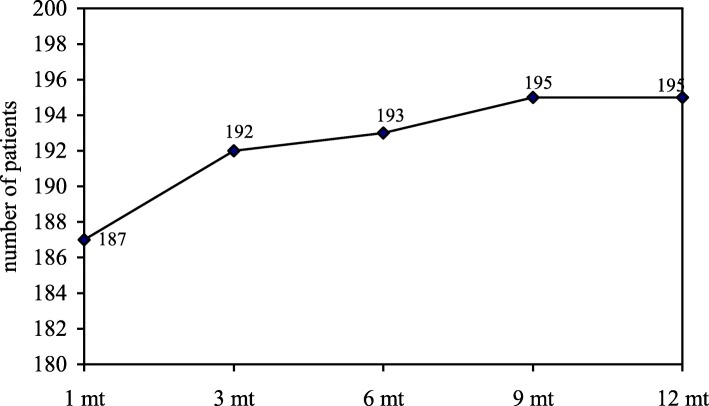
Results: A retrospective study is reported by evaluating 198 cases of ID from a single surgeon experience. All patients failed a previous conservative treatment. All cases were treated with the TAPP approach. Time to return to full sport activity was 4 weeks for 94.4% of patients, with a total of 98.5% of active patients at 9 months. Post-operative inguinal pain was the main complication (9.1%). On 13 years follow-up, we report a recurrence rate of 2.5%.
Conclusions: Current management algorithm for ID, in professional athletes, supports the role of surgery after at least 2 months of conservative treatment. Recently, the role of surgery has been highlighted for a definitive treatment and a faster full recovery to sport activity, especially for elite professional athletes. In our opinion, laparoscopic surgery is the mainstay for non-responsive ID treatment. We present a long-term retrospective evaluation of a wide cohort of professional athletes diagnosed and treated in a systematic way.
Keywords: Gilmore’s groin; Inguinal disruption; Mesh fixation; Sportsman’s groin; Sport’s hernia; Surgical glue; TAPP.
Conflict of interest statement
The authors, Guglielmo Niccolò Piozzi, Riccardo Cirelli, Ilaria Salati, Marco Enrico Mario Maino, Ennio Leopaldi, Giovanni Lenna, Franco Combi, and Giuseppe Massimiliano Sansonetti, declare that they have no competing interests.
Figures

References
LinkOut - more resources
Full Text Sources
