

Between-hospital variation in mortality and survival after glioblastoma surgery in the Dutch Quality Registry for Neuro Surgery
- PMID: 31236819
- PMCID: PMC6700042
- DOI: 10.1007/s11060-019-03229-5
Between-hospital variation in mortality and survival after glioblastoma surgery in the Dutch Quality Registry for Neuro Surgery
Abstract
Purpose: Standards for surgical decisions are unavailable, hence treatment decisions can be personalized, but also introduce variation in treatment and outcome. National registrations seek to monitor healthcare quality. The goal of the study is to measure between-hospital variation in risk-standardized survival outcome after glioblastoma surgery and to explore the association between survival and hospital characteristics in conjunction with patient-related risk factors.
Methods: Data of 2,409 adults with first-time glioblastoma surgery at 14 hospitals were obtained from a comprehensive, prospective population-based Quality Registry Neuro Surgery in The Netherlands between 2011 and 2014. We compared the observed survival with patient-specific risk-standardized expected early (30-day) mortality and late (2-year) survival, based on age, performance, and treatment year. We analyzed funnel plots, logistic regression and proportional hazards models.
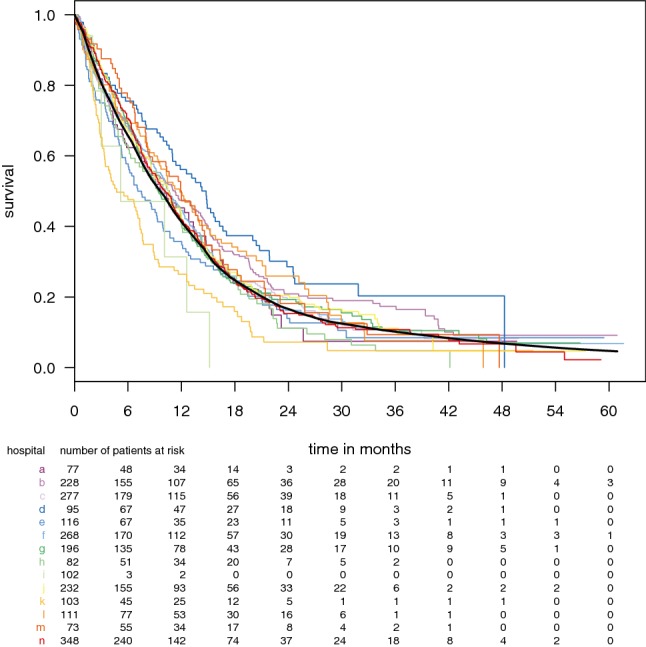
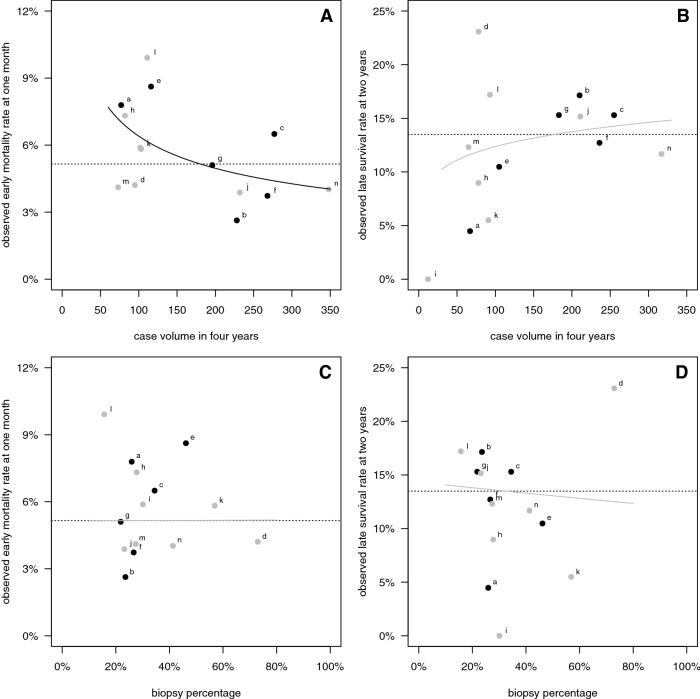
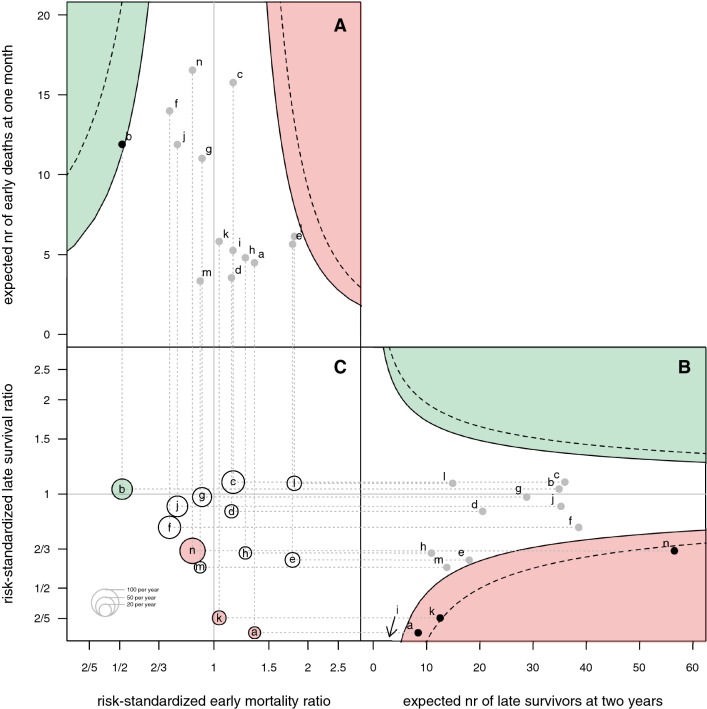
Results: Overall 30-day mortality was 5.2% and overall 2-year survival was 13.5%. Median survival varied between 4.8 and 14.9 months among hospitals, and biopsy percentages ranged between 16 and 73%. One hospital had lower than expected early mortality, and four hospitals had lower than expected late survival. Higher case volume was related with lower early mortality (P = 0.031). Patient-related risk factors (lower age; better performance; more recent years of treatment) were significantly associated with longer overall survival. Of the hospital characteristics, longer overall survival was associated with lower biopsy percentage (HR 2.09, 1.34-3.26, P = 0.001), and not with academic setting, nor with case volume.
Conclusions: Hospitals vary more in late survival than early mortality after glioblastoma surgery. Widely varying biopsy percentages indicate treatment variation. Patient-related factors have a stronger association with overall survival than hospital-related factors.
Keywords: Glioblastoma; Mortality; Neurosurgical procedures; Outcome assessment; Quality of health care; Survival.
Conflict of interest statement
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
