

Impact of Evidence-Based Stroke Care on Patient Outcomes: A Multilevel Analysis of an International Study
- PMID: 31237173
- PMCID: PMC6662356
- DOI: 10.1161/JAHA.119.012640
Impact of Evidence-Based Stroke Care on Patient Outcomes: A Multilevel Analysis of an International Study
Abstract
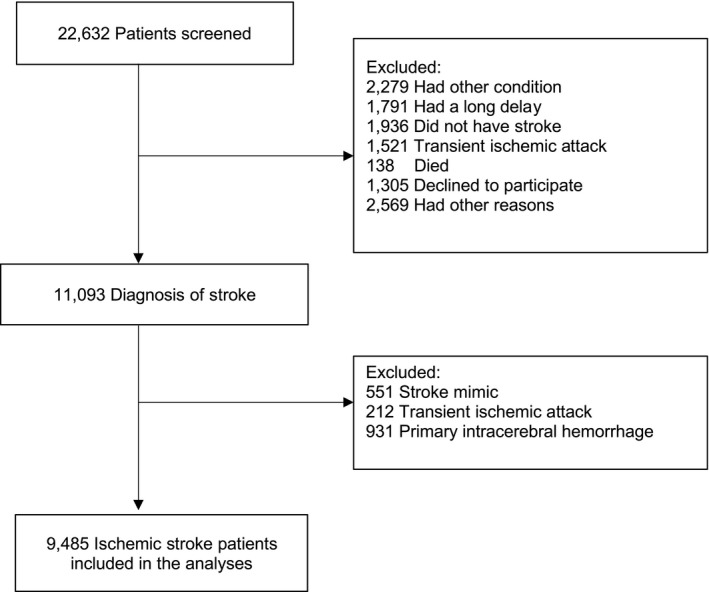
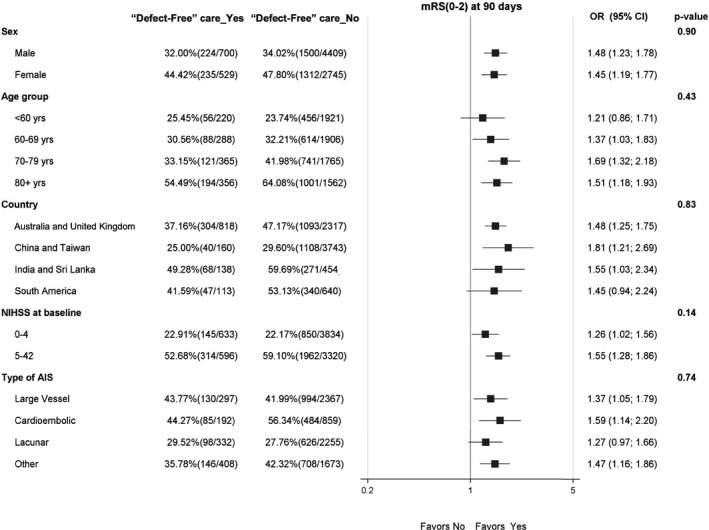
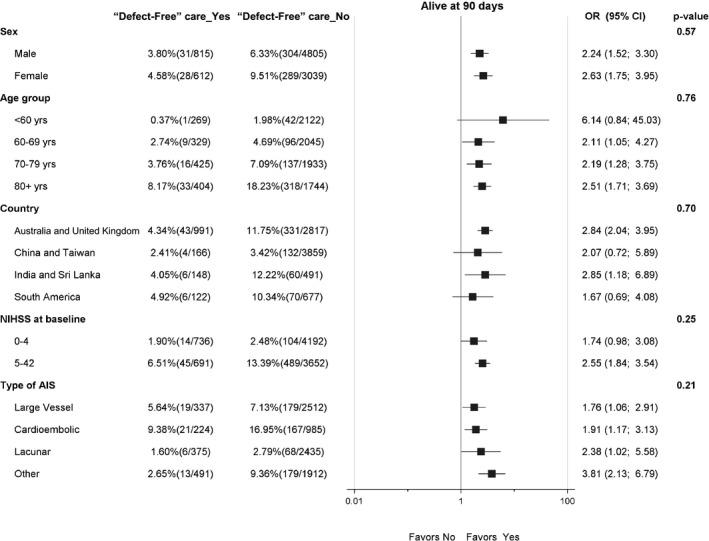
Background The uptake of proven stroke treatments varies widely. We aimed to determine the association of evidence-based processes of care for acute ischemic stroke ( AIS ) and clinical outcome of patients who participated in the HEADPOST (Head Positioning in Acute Stroke Trial), a multicenter cluster crossover trial of lying flat versus sitting up, head positioning in acute stroke. Methods and Results Use of 8 AIS processes of care were considered: reperfusion therapy in eligible patients; acute stroke unit care; antihypertensive, antiplatelet, statin, and anticoagulation for atrial fibrillation; dysphagia assessment; and physiotherapist review. Hierarchical, mixed, logistic regression models were performed to determine associations with good outcome (modified Rankin Scale scores 0-2) at 90 days, adjusted for patient and hospital variables. Among 9485 patients with AIS, implementation of all processes of care in eligible patients, or "defect-free" care, was associated with improved outcome (odds ratio, 1.40; 95% CI, 1.18-1.65) and better survival (odds ratio, 2.23; 95% CI , 1.62-3.09). Defect-free stroke care was also significantly associated with excellent outcome (modified Rankin Scale score 0-1) (odds ratio, 1.22; 95% CI , 1.04-1.43). No hospital characteristic was independently predictive of outcome. Only 1445 (15%) of eligible patients with AIS received all processes of care, with significant regional variations in overall and individual rates. Conclusions Use of evidence-based care is associated with improved clinical outcome in AIS . Strategies are required to address regional variation in the use of proven AIS treatments. Clinical Trial Registration URL : https://www.clinicaltrials.gov . Unique Identifier: NCT02162017.
Keywords: acute stroke care; multilevel analysis; outcome; quality.
Figures
References
-
- Bray BD, Paley L, Hoffman A, James M, Gompertz P, Wolfe CDA, Hemingway H, Rudd AG; SSNAP Collaboration . Socioeconomic disparities in first stroke incidence, quality of care, and survival: a nationwide registry‐based cohort study of 44 million adults in England. Lancet Public Health. 2018;3:e185–e193. - PMC - PubMed
-
- Glader EL, Stegmayr B, Johansson L, Hulter‐Åsberg K, Wester PO. Differences in long‐term outcome between patients treated in stroke units and in general wards: a 2‐year follow‐up of stroke patients in Sweden. Stroke 2001;32:2124–213. - PubMed
-
- Saposnik G, Kapral MK, Coutts SB, Fang J, Demchuk AM, Hill MD; the investigators of the Registry of the Canadian Stroke Network (RCSN) for the Stroke Outcome Research Canada (SORCan) Working Group . Do all age groups benefit from organized inpatient stroke care?. Stroke 2009;40:3321–3327. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
