

Discriminative Accuracy of FEV1:FVC Thresholds for COPD-Related Hospitalization and Mortality
- PMID: 31237643
- PMCID: PMC6593636
- DOI: 10.1001/jama.2019.7233
Discriminative Accuracy of FEV1:FVC Thresholds for COPD-Related Hospitalization and Mortality
Abstract
Importance: According to numerous current guidelines, the diagnosis of chronic obstructive pulmonary disease (COPD) requires a ratio of the forced expiratory volume in the first second to the forced vital capacity (FEV1:FVC) of less than 0.70, yet this fixed threshold is based on expert opinion and remains controversial.
Objective: To determine the discriminative accuracy of various FEV1:FVC fixed thresholds for predicting COPD-related hospitalization and mortality.
Design, setting, and participants: The National Heart, Lung, and Blood Institute (NHLBI) Pooled Cohorts Study harmonized and pooled data from 4 US general population-based cohorts (Atherosclerosis Risk in Communities Study; Cardiovascular Health Study; Health, Aging, and Body Composition Study; and Multi-Ethnic Study of Atherosclerosis). Participants aged 45 to 102 years were enrolled from 1987 to 2000 and received follow-up longitudinally through 2016.
Exposures: Presence of airflow obstruction, which was defined by a baseline FEV1:FVC less than a range of fixed thresholds (0.75 to 0.65) or less than the lower limit of normal as defined by Global Lung Initiative reference equations (LLN).
Main outcomes and measures: The primary outcome was a composite of COPD hospitalization and COPD-related mortality, defined by adjudication or administrative criteria. The optimal fixed FEV1:FVC threshold was defined by the best discrimination for these COPD-related events as indexed using the Harrell C statistic from unadjusted Cox proportional hazards models. Differences in C statistics were compared with respect to less than 0.70 and less than LLN thresholds using a nonparametric approach.
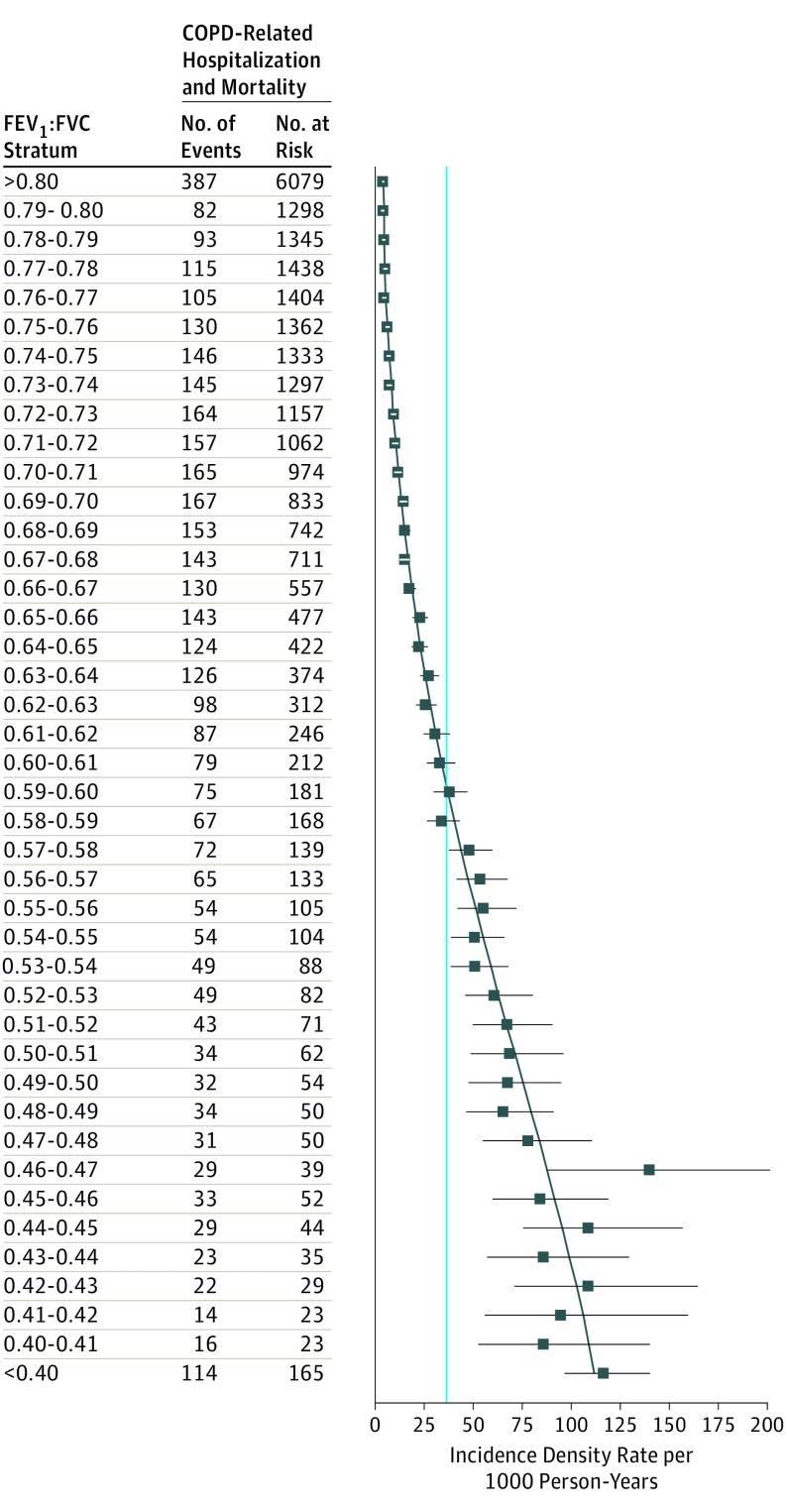
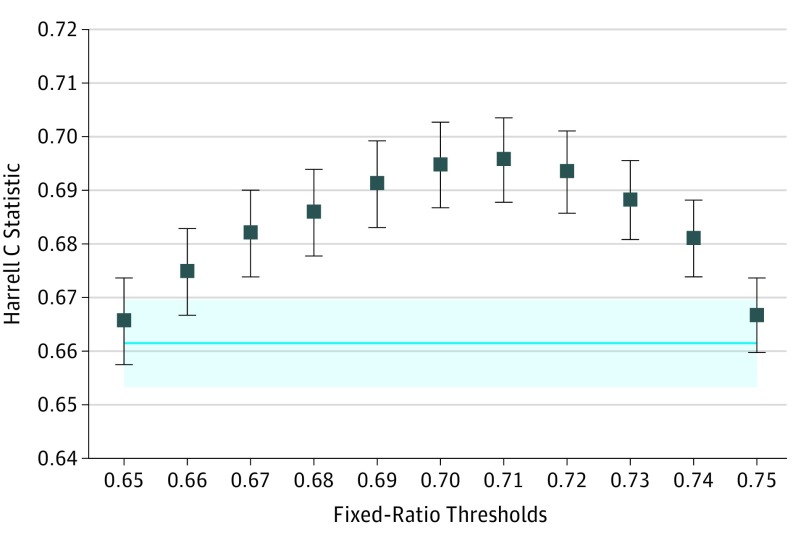
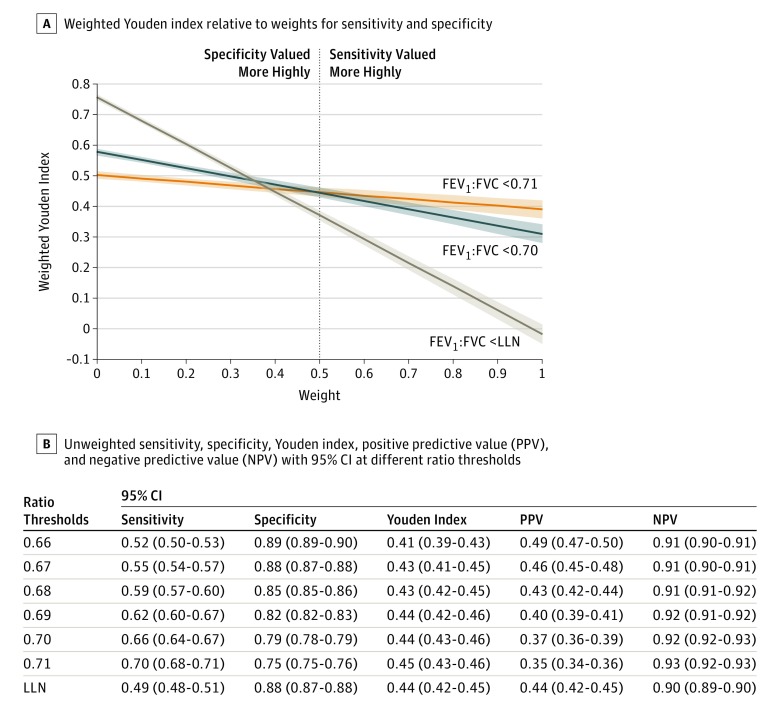
Results: Among 24 207 adults in the pooled cohort (mean [SD] age at enrollment, 63 [10.5] years; 12 990 [54%] women; 16 794 [69%] non-Hispanic white; 15 181 [63%] ever smokers), complete follow-up was available for 11 077 (77%) at 15 years. During a median follow-up of 15 years, 3925 participants experienced COPD-related events over 340 757 person-years of follow-up (incidence density rate, 11.5 per 1000 person-years), including 3563 COPD-related hospitalizations and 447 COPD-related deaths. With respect to discrimination of COPD-related events, the optimal fixed threshold (0.71; C statistic for optimal fixed threshold, 0.696) was not significantly different from the 0.70 threshold (difference, 0.001 [95% CI, -0.002 to 0.004]) but was more accurate than the LLN threshold (difference, 0.034 [95% CI, 0.028 to 0.041]). The 0.70 threshold provided optimal discrimination in the subgroup analysis of ever smokers and in adjusted models.
Conclusions and relevance: Defining airflow obstruction as FEV1:FVC less than 0.70 provided discrimination of COPD-related hospitalization and mortality that was not significantly different or was more accurate than other fixed thresholds and the LLN. These results support the use of FEV1:FVC less than 0.70 to identify individuals at risk of clinically significant COPD.
Conflict of interest statement
Figures
Comment in
-
Accuracy of Airflow Obstruction Thresholds for Predicting COPD-Related Hospitalization and Mortality: Can Simple Diagnostic Thresholds Be Used for a Complex Disease?JAMA. 2019 Jun 25;321(24):2412-2413. doi: 10.1001/jama.2019.6584. JAMA. 2019. PMID: 31237620 No abstract available.
-
FEV1:FVC Thresholds for Defining Chronic Obstructive Pulmonary Disease.JAMA. 2019 Oct 22;322(16):1610-1611. doi: 10.1001/jama.2019.13945. JAMA. 2019. PMID: 31638668 No abstract available.
-
FEV1:FVC Thresholds for Defining Chronic Obstructive Pulmonary Disease.JAMA. 2019 Oct 22;322(16):1609-1610. doi: 10.1001/jama.2019.13948. JAMA. 2019. PMID: 31638669 No abstract available.
-
FEV1:FVC Thresholds for Defining Chronic Obstructive Pulmonary Disease.JAMA. 2019 Oct 22;322(16):1611. doi: 10.1001/jama.2019.13957. JAMA. 2019. PMID: 31638671 No abstract available.
-
Kommentar zu S. Meinrenken. COPD-Diagnose: FEV1:FVC-Grenzwert bestätigt sich in großen Studien. Pneumologie 2020; 74: 10.Pneumologie. 2020 May;74(5):259. doi: 10.1055/a-1140-2941. Epub 2020 May 11. Pneumologie. 2020. PMID: 32392614 German. No abstract available.
References
-
- Collaborators GBDCRD; GBD 2015 Chronic Respiratory Disease Collaborators . Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(9):691-706. doi: 10.1016/S2213-2600(17)30293-X - DOI - PMC - PubMed
-
- Mannino DM, Homa DM, Akinbami LJ, Ford ES, Redd SC. Chronic obstructive pulmonary disease surveillance—United States, 1971-2000. MMWR Surveill Summ. 2002;51(6):1-16. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AG023629/AG/NIA NIH HHS/United States
- U01 HL130114/HL/NHLBI NIH HHS/United States
- N01HC95168/HL/NHLBI NIH HHS/United States
- R01 HL093081/HL/NHLBI NIH HHS/United States
- N01HC95165/HL/NHLBI NIH HHS/United States
- N01HC95167/HL/NHLBI NIH HHS/United States
- N01HC95159/HL/NHLBI NIH HHS/United States
- N01HC95163/HL/NHLBI NIH HHS/United States
- R21 HL129924/HL/NHLBI NIH HHS/United States
- N01HC95164/HL/NHLBI NIH HHS/United States
- R01 HL130506/HL/NHLBI NIH HHS/United States
- N01HC95166/HL/NHLBI NIH HHS/United States
- K23 HL130627/HL/NHLBI NIH HHS/United States
- N01HC95160/HL/NHLBI NIH HHS/United States
- R01 HL122477/HL/NHLBI NIH HHS/United States
- RC1 HL100543/HL/NHLBI NIH HHS/United States
- N01HC95169/HL/NHLBI NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01HC95161/HL/NHLBI NIH HHS/United States
- K23 HL133438/HL/NHLBI NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- K24 HL140108/HL/NHLBI NIH HHS/United States
- UL1 TR001409/TR/NCATS NIH HHS/United States
- N01HC95162/HL/NHLBI NIH HHS/United States
- R01 AG028050/AG/NIA NIH HHS/United States
- R01 NR012459/NR/NINR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
