

Aspirin for primary prevention of stroke in individuals without cardiovascular disease-A meta-analysis
- PMID: 31237833
- PMCID: PMC7003154
- DOI: 10.1177/1747493019858780
Aspirin for primary prevention of stroke in individuals without cardiovascular disease-A meta-analysis
Abstract
Background: The benefits of aspirin for primary prevention of stroke are uncertain.
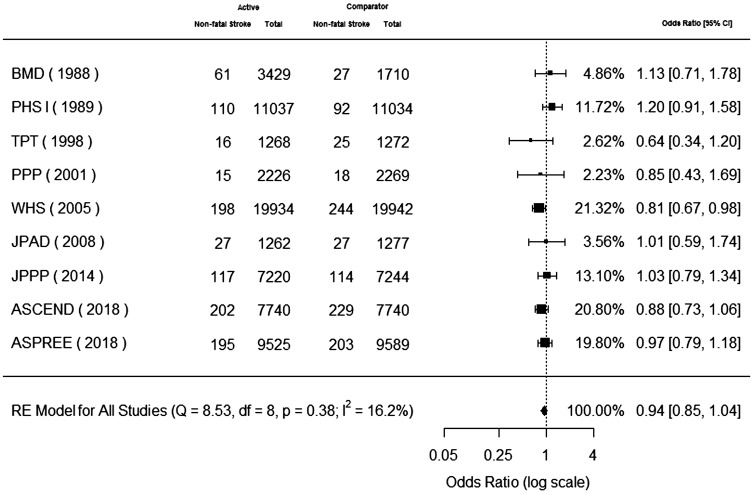
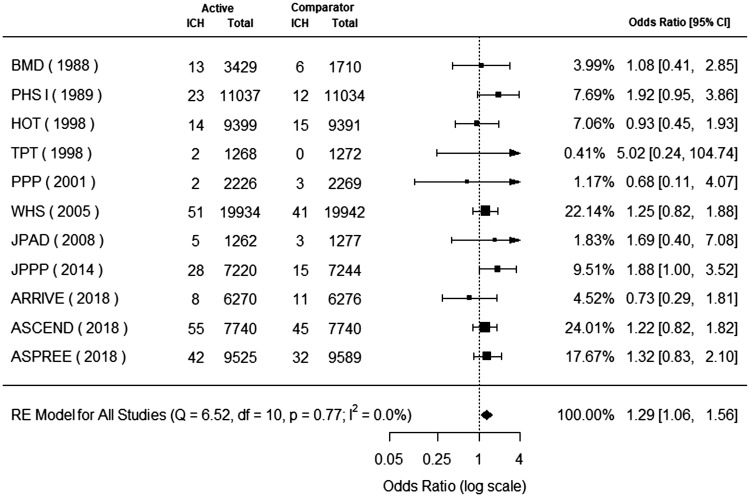
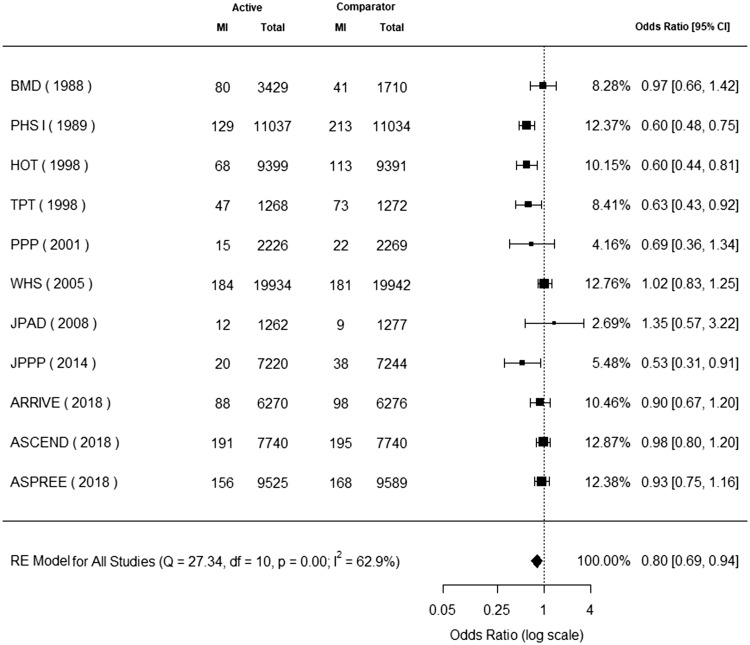
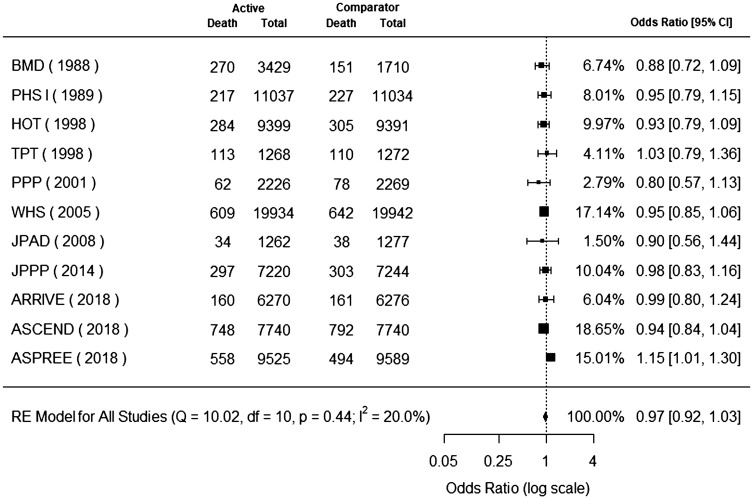
Methods: We performed a cumulative meta-analysis of trials investigating aspirin for primary prevention of cardiovascular disease with a focus on stroke. We assessed the effects of aspirin on non-fatal stroke, hemorrhagic stroke, non-fatal myocardial infarction, all-cause mortality, cardiovascular mortality, major gastrointestinal bleeding, and an analysis of net clinical effect, in populations without a history of clinical or subclinical cardiovascular disease.
Summary of review results: Among 11 trials (157,054 participants), aspirin was not associated with a statistically significant reduction in non-fatal stroke (odds ratio, 0.94; 95% CI, 0.85 to 1.04) but was associated with an increased risk of hemorrhagic stroke (odds ratio, 1.29; 95% CI, 1.06 to 1.56). Aspirin was not associated with a statistically significant reduction in all-cause mortality (odds ratio, 0.97; 95% CI, 0.92 to 1.03) or cardiovascular mortality (odds ratio, 0.94; 95% CI, 0.85 to 1.03). Aspirin was associated with a reduction in non-fatal myocardial infarction (odds ratio, 0.80; 95% CI, 0.69 to 0.94) and an increased risk of major gastrointestinal bleeding (odds ratio, 1.83; 95% CI, 1.43 to 2.35). Using equal weighting for non-fatal events and major bleeding, we observed no net clinical benefit with aspirin use for primary prevention.
Conclusion: Our meta-analysis reports no benefit of aspirin for primary stroke prevention.
Keywords: Stroke; aspirin; cardiovascular; prevention.
Figures
References
-
- Cleland JGF. Is aspirin useful in primary prevention?. Eur Heart J 2013; 34: 3412–3418. - PubMed
-
- Williams CD, Chan AT, Elman MR, et al. Aspirin use among adults in the U.S. Am J Prev Med 2015; 48: 501–508. - PubMed
-
- Bibbins-Domingo K. on behalf of the U.S. Preventive Services Task Force. Aspirin use for the primary prevention of cardiovascular disease and colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2016; 164: 836. - PubMed
-
- Whitlock EP, Burda BU, Williams SB, Guirguis-Blake JM, Evans CV. Bleeding risks with aspirin use for primary prevention in adults: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med 2016; 164: 826. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
