

Rapid Apparent Diffusion Coefficient Evolution After Early Revascularization
- PMID: 31238830
- PMCID: PMC6646065
- DOI: 10.1161/STROKEAHA.119.025784
Rapid Apparent Diffusion Coefficient Evolution After Early Revascularization
Erratum in
-
Correction to: Rapid Apparent Diffusion Coefficient Evolution After Early Revascularization: A Potential Marker of Secondary Injury?Stroke. 2019 Sep;50(9):e282. doi: 10.1161/STR.0000000000000206. Epub 2019 Aug 26. Stroke. 2019. PMID: 31449484 No abstract available.
Abstract
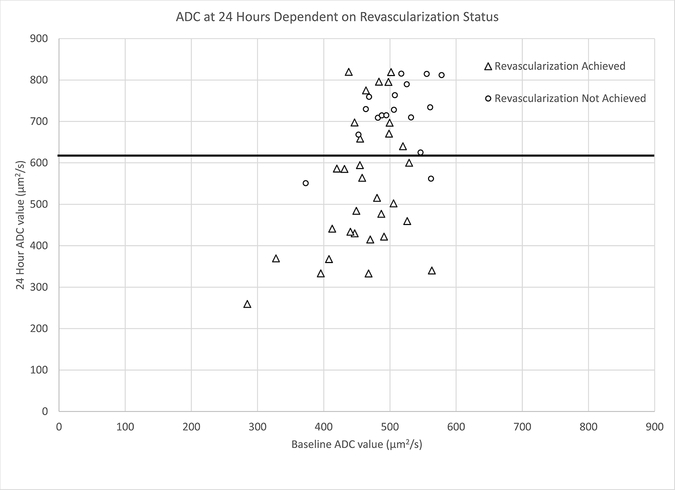
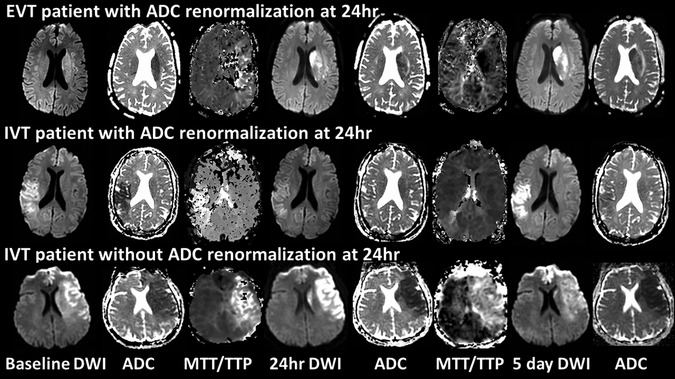
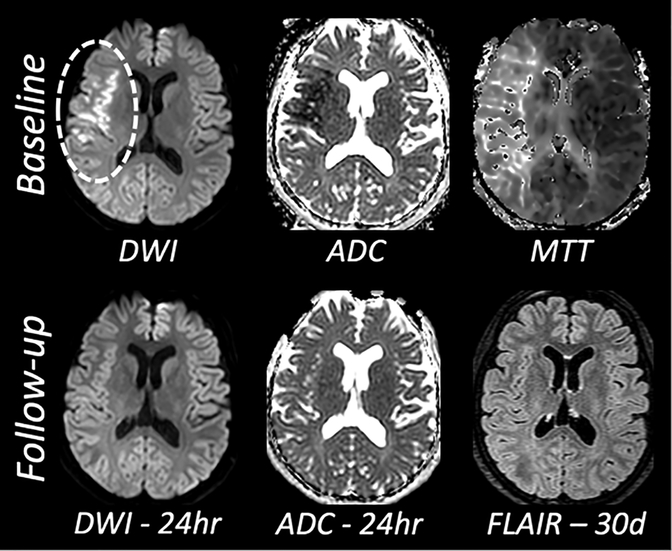
Background and Purpose- In this era of endovascular therapy (EVT) with early, complete recanalization and reperfusion, we have observed an even more rapid apparent diffusion coefficient (ADC) normalization within the acute ischemic lesion compared with the natural history or IV-tPA-treated patient. In this study, we aimed to evaluate the effect of revascularization on ADC evolution within the core lesion in the first 24 hours in acute ischemic stroke patients. Methods- This retrospective study included anterior circulation acute ischemic stroke patients treated with EVT with or without intravenous tPA (IVT) from 2015 to 2017 compared with a consecutive cohort of IVT-only patients treated before 2015. Diffusion-weighted imaging and ADC maps were used to quantify baseline core lesions. Median ADC value change and core reversal were determined at 24 hours. Diffusion-weighted imaging lesion growth was measured at 24 hours and 5 days. Good clinical outcome was defined as modified Rankin Scale score of 0 to 2 at 90 days. Results- Twenty-five patients (50%) received IVT while the other 25 patients received EVT (50%) with or without IVT. Between these patient groups, there were no differences in age, sex, baseline National Institutes of Health Stroke Scale, interhospital transfer, or IVT rates. Thirty-two patients (64%) revascularized with 69% receiving EVT. There was a significant increase in median ADC value of the core lesion at 24 hours in patients who revascularized compared with further ADC reduction in nonrevascularization patients. Revascularization patients had a significantly higher rate of good clinical outcome at 90 days, 63% versus 9% (P=0.003). Core reversal at 24 hours was significantly higher in revascularization patients, 69% versus 22% (P=0.002). Conclusions- ADC evolution in acute ischemic stroke patients with early, complete revascularization, now more commonly seen with EVT, is strikingly different from our historical understanding. The early ADC normalization we have observed in this setting may include a component of secondary injury and serve as a potential imaging biomarker for the development of future adjunctive therapies. Clinical Trial Registration- URL: https://www.clinicaltrials.gov. Unique identifier: NCT00009243.
Keywords: biomarkers; embolectomy; ischemia; magnetic resonance imaging; reperfusion; stroke.
Conflict of interest statement
Conflicts of Interest/Disclosures
All authors: None.
Figures
References
-
- Baird AE, Warach S. Magnetic resonance imaging of acute stroke. J Cereb Blood Flow Metab. 1998;18:583–609 - PubMed
-
- Schuier FJ, Hossmann KA. Experimental brain infarcts in cats. Ii. Ischemic brain edema. Stroke. 1980;11:593–601 - PubMed
-
- Norris DG, Niendorf T, Leibfritz D. Health and infarcted brain tissues studied at short diffusion times: The origins of apparent restriction and the reduction in apparent diffusion coefficient. NMR Biomed. 1994;7:304–310 - PubMed
-
- Schlaug G, Benfield A, Baird AE, Siewert B, Lovblad KO, Parker RA, et al. The ischemic penumbra: Operationally defined by diffusion and perfusion mri. Neurology. 1999;53:1528–1537 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
