

Survival and death causes of patients with giant cell arteritis in Western Norway 1972-2012: a retrospective cohort study
- PMID: 31238961
- PMCID: PMC6593490
- DOI: 10.1186/s13075-019-1945-4
Survival and death causes of patients with giant cell arteritis in Western Norway 1972-2012: a retrospective cohort study
Abstract
Background: Our objective was to determine the survival and causes of death in a large and well-characterized cohort of patients with giant cell arteritis (GCA).
Methods: This is a hospital-based, retrospective, observational cohort study including patients diagnosed with GCA in Western Norway during 1972-2012. Patients were identified through computerized hospital records using the International Classification of Diseases (ICD)-coding system. Medical records were reviewed. Patients were randomly assigned population controls matched on age, sex, and geography from the Central Population Registry of Norway (CPRN). Date and cause of death were obtained from the Norwegian Cause of Death Registry (NCoDR). The survival was analyzed using Kaplan-Meier methods with the Gehan-Breslow test and the causes of death using cumulative incidence and Cox models for competing risks.
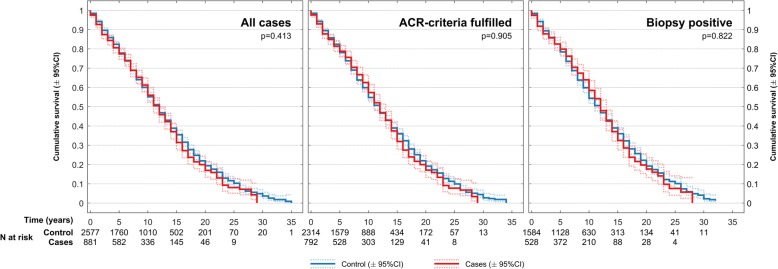
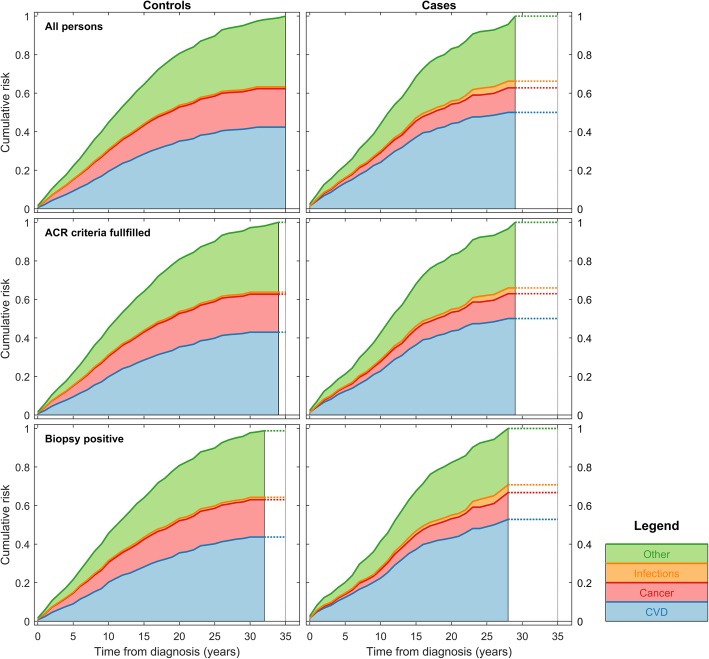
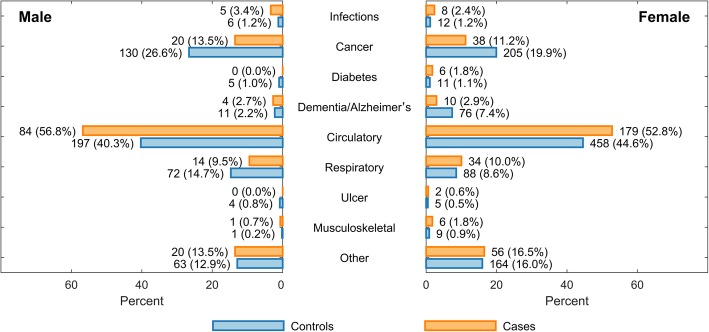
Results: We identified 881 cases with a clinical diagnosis of GCA of which 792 fulfilled the American College of Rheumatology (ACR) 1990 classification criteria. Among those fulfilling the ACR criteria, 528 were also biopsy-verified. Cases were matched with 2577 population controls. A total of 490 (56%) GCA patients and 1517 (59%) controls died during the study period. We found no difference in the overall survival of GCA patients compared to controls, p = 0.413. The most frequent underlying causes of death in both groups were diseases of the circulatory system followed by cancer. GCA patients had increased risk of dying of circulatory disease (HR 1.31, 95% CI 1.13-1.51, p < 0.001) but lower risk of dying of cancer (HR 0.56, 95% CI 0.42-0.73, p < 0.001) compared to population controls.
Conclusions: We found no difference in the overall survival of GCA patients compared to matched controls, but there were differences in the distribution of underlying death causes.
Keywords: Causes of death; Epidemiology; Giant cell arteritis; Mortality; Survival; Temporal arteritis; Vasculitis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
