

Nivolumab in Patients with Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck: Efficacy and Safety in CheckMate 141 by Prior Cetuximab Use
- PMID: 31239321
- PMCID: PMC7721346
- DOI: 10.1158/1078-0432.CCR-18-3944
Nivolumab in Patients with Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck: Efficacy and Safety in CheckMate 141 by Prior Cetuximab Use
Abstract
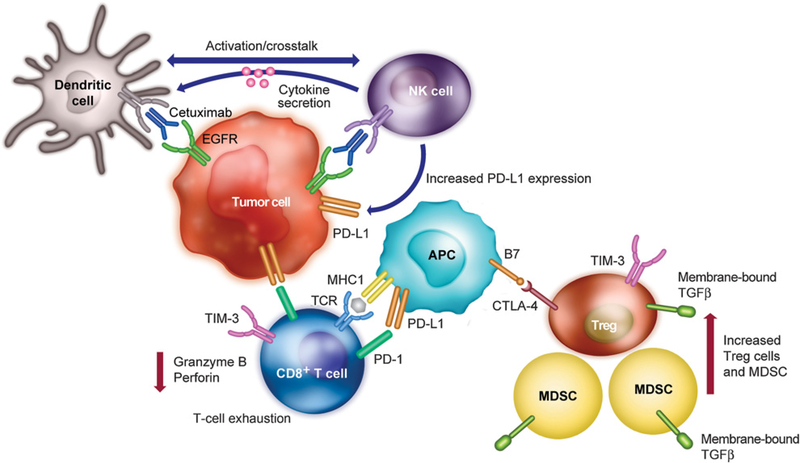
Purpose: Cetuximab, which modulates immune responses, may affect the efficacy of subsequent immunotherapy. Here, we assessed outcomes with nivolumab, by prior cetuximab exposure, in patients with recurrent or metastatic (R/M) squamous cell carcinoma of the head and neck (SCCHN) who had experienced progression within 6 months of platinum-containing chemotherapy.
Patients and methods: In the randomized, open-label, phase III CheckMate 141 trial, patients were randomized 2:1 to nivolumab 3 mg/kg every 2 weeks or investigator's choice (IC) of single-agent chemotherapy, with stratification by prior cetuximab exposure. The primary endpoint was overall survival (OS); additional endpoints were progression-free survival, objective response rate, and safety.
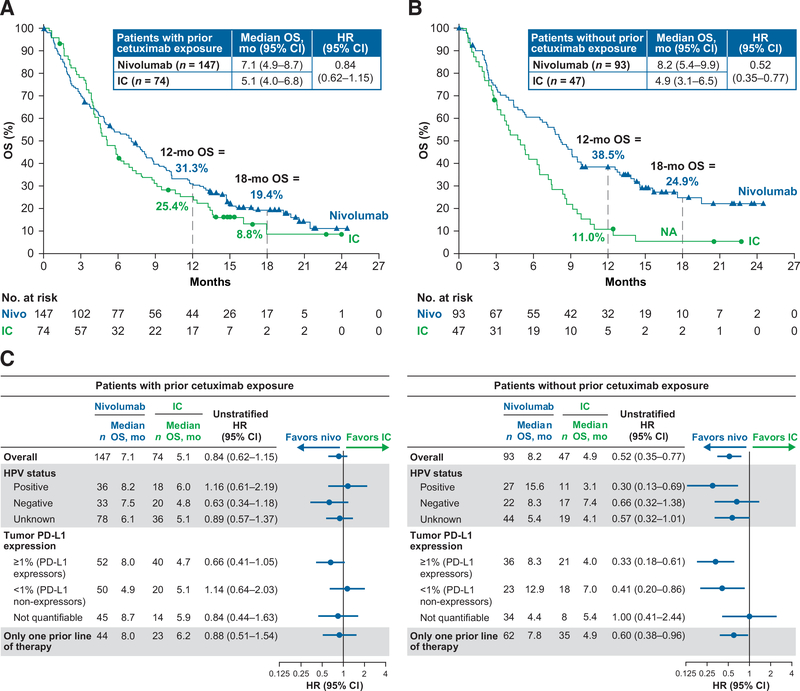
Results: In patients with prior cetuximab exposure, the median OS was 7.1 months with nivolumab versus 5.1 months with IC (HR, 0.84; 95% CI, 0.62-1.15); OS benefit with nivolumab was maintained across most demographic subgroups. In patients without prior cetuximab exposure, the median OS was 8.2 months with nivolumab versus 4.9 months with IC (HR, 0.52; 95% CI, 0.35-0.77); OS benefit with nivolumab was maintained across patient baseline subgroups including tumor programmed death ligand 1 (PD-L1) expression (<1% or ≥1%). Grade 3-4 treatment-related adverse event rates favored nivolumab versus IC in both subgroups.
Conclusions: Nivolumab appeared to improve efficacy versus IC regardless of prior cetuximab use, supporting its use in patients with R/M SCCHN with or without prior cetuximab exposure. The reduction in risk of death with nivolumab compared with IC was greater in patients without prior cetuximab exposure versus with prior cetuximab exposure.
©2019 American Association for Cancer Research.
Figures
References
-
- de Andrade DA, Machiels JP. Treatment options for patients with recurrent or metastatic squamous cell carcinoma of the head and neck, who progress after platinum-based chemotherapy. Curr Opin Oncol 2012;24:211–7. - PubMed
-
- KEYTRUDA (pembrolizumab) for injection, for intravenous use [prescribing information]. Whitehouse Station, NJ: Merck & Co., Inc.; 2017.
-
- OPDIVO (nivolumab) injection, for intravenous use [prescribing information]. Princeton, NJ: Bristol-Myers Squibb; 2017.
-
- Mendelsohn J, Baselga J. Status of epidermal growth factor receptor antagonists in the biology and treatment of cancer. J Clin Oncol 2003; 21:2787–99. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
