Mechanical thrombectomy for basilar artery occlusion: efficacy, outcomes, and futile recanalization in comparison with the anterior circulation
- PMID: 31239331
- PMCID: PMC6902072
- DOI: 10.1136/neurintsurg-2018-014516
Mechanical thrombectomy for basilar artery occlusion: efficacy, outcomes, and futile recanalization in comparison with the anterior circulation
Abstract
Background: Performing mechanical thrombectomy (MT) in patients with basilar artery occlusion (BAO) is currently not evidence-based.
Objective: To compare patients' outcome, relative merits of achieving recanalization, and predictors of futile recanalization (FR) between BAO and anterior circulation large vessel occlusion (ACLVO) MT.
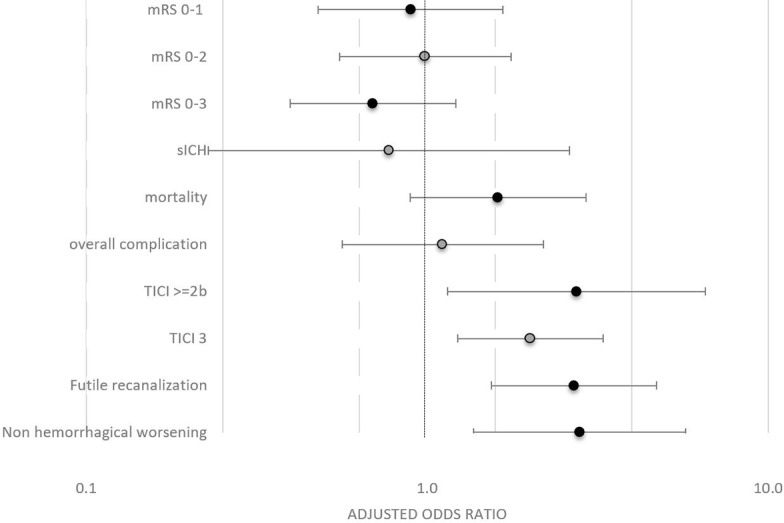
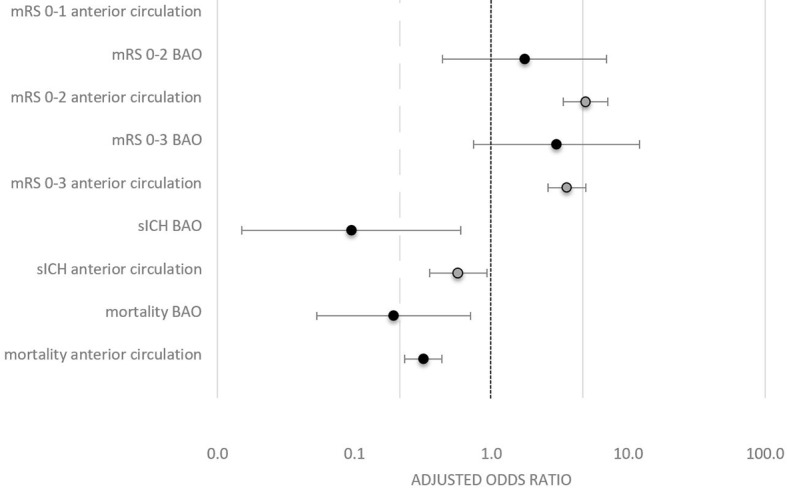
Methods: In the multicenter BEYOND-SWIFT registry (NCT03496064), univariate and multivariate (displayed as adjusted Odds Ratios, aOR and 95% confidence intervals, 95%-CI) outcome comparisons between BAO (N=165) and ACLVO (N=1574) were performed. The primary outcome was favorable outcome at 90 days (modified Rankin Scale, mRS 0-2). Secondary outcome included mortality, symptomatic intracranial hemorrhage (sICH) and FR. The relative merits of achieving successful recanalization between ACLVO and BAO were evaluated with interaction terms.
Results: MT in BAO was more often technically effective and equally safe in regards to mortality and sICH when compared to ACLVO. When adjusting for baseline differences, there was no significant difference between BAO vs ACLVO regarding rates of favorable outcome (aOR 0.986, 95%-CI 0.553 - 1.758). However, BAO were associated with increased rates of FR (aOR 2.146, 95%-CI 1.267 - 3.633). Predictors for FR were age, stroke severity, maneuver count and intracranial stenting. No significant heterogeneity on the relative merits of achieving successful recanalization on several outcome parameters were observed when comparing BAO and ACLVO.
Conclusions: In selected patients, similar outcomes can be achieved in BAO and ACLVO patients treated with MT. Randomized controlled trials comparing patient selection and interventional strategies seem warranted to avoid FR.
Trial registration number: NCT03496064.
Keywords: angiography; intervention; stroke; thrombectomy; thrombolysis.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: UF is a consultant for Medtronic and Stryker and co-principal investigator of the SWIFT DIRECT trial (Medtronic). JG is a global principal investigator of STAR (Solitaire FR Thrombectomy for Acute Revascularisation), clinical event commitee member of the PROMISE study (European Registry on the ACE Reperfusion Catheters and the Penumbra System in the Treatment of Acute Ischemic Stroke; Penumbra), and a principal investigator and consultant for the SWIFT DIRECT study (Medtronic) and receives Swiss National Science Foundation (SNSF) grants for magnetic resonance imaging in stroke. LPi serves as a consultant for Balt, Microvention, and Penumbra. JK has received travel grants from Pfizer and Stryker. MRi serves as a consultant for Medtronic, Stryker, Anaconda, Apta Targets, and Perflow Medical and as a speaker for Neuravi. PMi has received funding for speaker honoraria from Boehringer. He has served on scientific advisory boards also for Boehringer. He has received research grants from Bristol-Myers Squibb, Boehringer, and the Swiss Heart Foundation. VMP is a consultant for Stryker (SC for DAWN trial), Penumbra (SC for PROMISE study), BALT (proctorship of products unrelated to ischemic stroke), Phenox, Rapid Medical, Neurovasc and receives research a grant from Philips. All the other authors have nothing to disclose.
Figures