

A comprehensive, multiscale framework for evaluation of arrhythmias arising from cell therapy in the whole post-myocardial infarcted heart
- PMID: 31239508
- PMCID: PMC6592890
- DOI: 10.1038/s41598-019-45684-0
A comprehensive, multiscale framework for evaluation of arrhythmias arising from cell therapy in the whole post-myocardial infarcted heart
Abstract
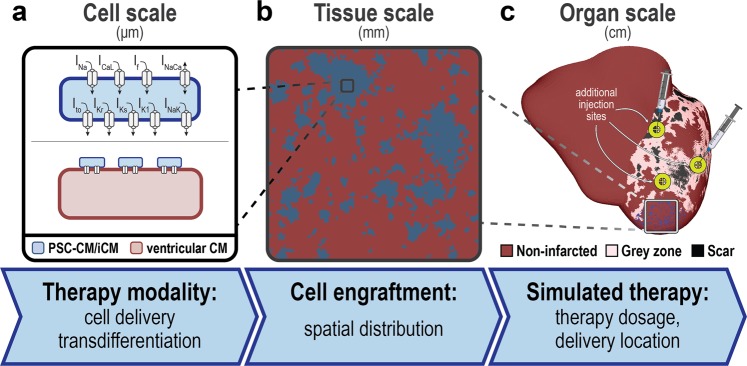
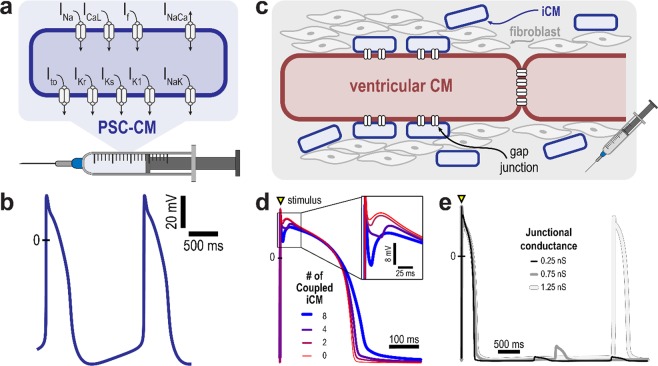
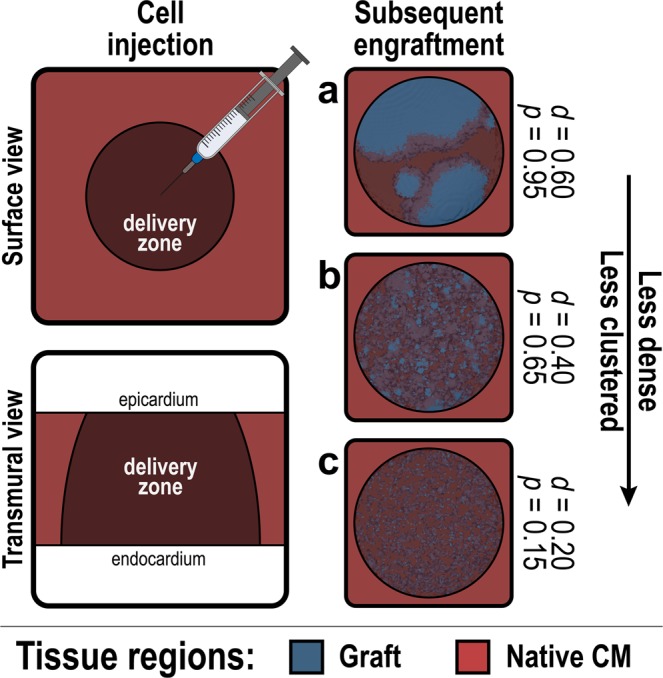
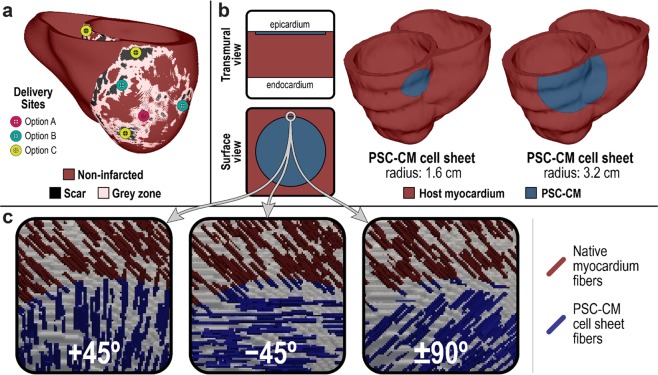
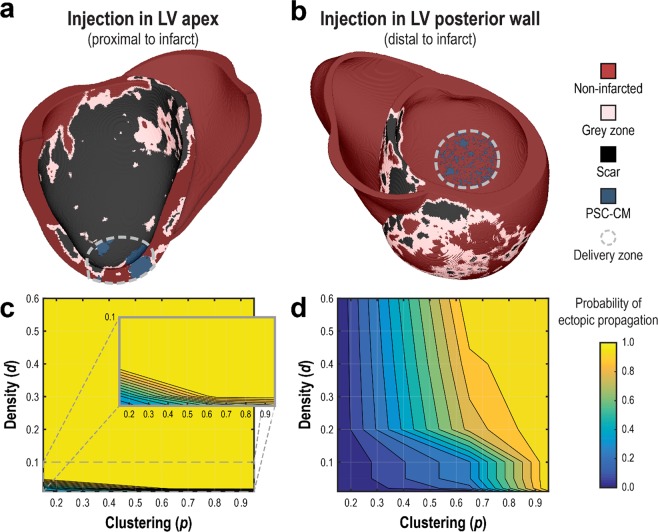
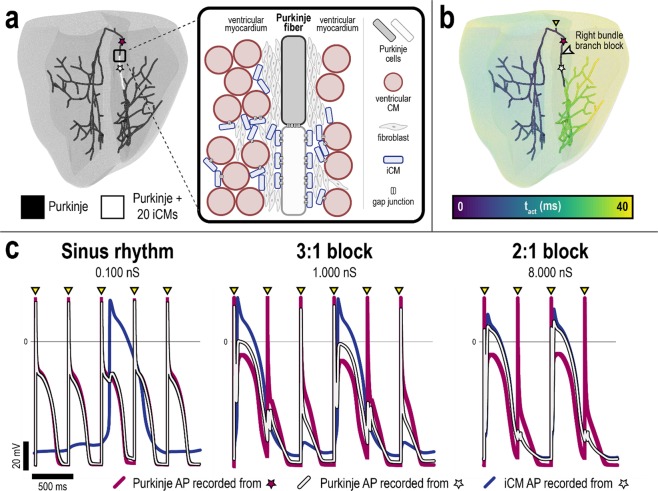
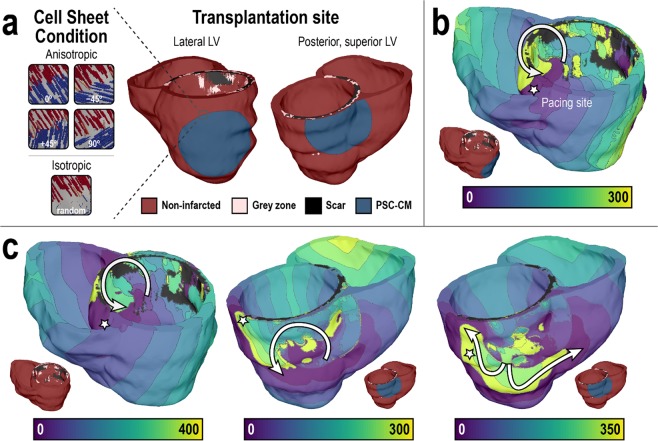
Direct remuscularization approaches to cell-based heart repair seek to restore ventricular contractility following myocardial infarction (MI) by introducing new cardiomyocytes (CMs) to replace lost or injured ones. However, despite promising improvements in cardiac function, high incidences of ventricular arrhythmias have been observed in animal models of MI injected with pluripotent stem cell-derived cardiomyocytes (PSC-CMs). The mechanisms of arrhythmogenesis remain unclear. Here, we present a comprehensive framework for computational modeling of direct remuscularization approaches to cell therapy. Our multiscale 3D whole-heart modeling framework integrates realistic representations of cell delivery and transdifferentiation therapy modalities as well as representation of spatial distributions of engrafted cells, enabling simulation of clinical therapy and the prediction of emergent electrophysiological behavior and arrhythmogenensis. We employ this framework to explore how varying parameters of cell delivery and transdifferentiation could result in three mechanisms of arrhythmogenesis: focal ectopy, heart block, and reentry.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Assessment of arrhythmia mechanism and burden of the infarcted ventricles following remuscularization with pluripotent stem cell-derived cardiomyocyte patches using patient-derived models.Cardiovasc Res. 2022 Mar 25;118(5):1247-1261. doi: 10.1093/cvr/cvab140. Cardiovasc Res. 2022. PMID: 33881518 Free PMC article.
-
Human Embryonic Stem Cell-Derived Cardiomyocytes Regenerate the Infarcted Pig Heart but Induce Ventricular Tachyarrhythmias.Stem Cell Reports. 2019 May 14;12(5):967-981. doi: 10.1016/j.stemcr.2019.04.005. Epub 2019 May 2. Stem Cell Reports. 2019. PMID: 31056479 Free PMC article.
-
Robust Cardiac Regeneration: Fulfilling the Promise of Cardiac Cell Therapy.Clin Ther. 2020 Oct;42(10):1857-1879. doi: 10.1016/j.clinthera.2020.08.008. Epub 2020 Sep 14. Clin Ther. 2020. PMID: 32943195 Review.
-
Pharmacologic therapy for engraftment arrhythmia induced by transplantation of human cardiomyocytes.Stem Cell Reports. 2021 Oct 12;16(10):2473-2487. doi: 10.1016/j.stemcr.2021.08.005. Epub 2021 Sep 9. Stem Cell Reports. 2021. PMID: 34506727 Free PMC article.
-
Pluripotent Stem Cell-Derived Cardiomyocyte Transplantation for Heart Disease Treatment.Curr Cardiol Rep. 2019 Jun 21;21(8):73. doi: 10.1007/s11886-019-1171-3. Curr Cardiol Rep. 2019. PMID: 31228011 Review.
Cited by
-
Computational modeling of cardiac electrophysiology and arrhythmogenesis: toward clinical translation.Physiol Rev. 2024 Jul 1;104(3):1265-1333. doi: 10.1152/physrev.00017.2023. Epub 2023 Dec 28. Physiol Rev. 2024. PMID: 38153307 Free PMC article. Review.
-
Leave the light on: chronic optogenetic tachypacing of human engineered cardiac tissue constructs.Cardiovasc Res. 2020 Jul 1;116(8):1405-1406. doi: 10.1093/cvr/cvaa029. Cardiovasc Res. 2020. PMID: 32031599 Free PMC article. No abstract available.
-
Computational Simulations Show Proof-of-Concept for Optogenetic Suppression of Ectopic Activity in Cardiac Stem Cell Therapy.Cardiovasc Eng Technol. 2025 Jul 16. doi: 10.1007/s13239-025-00794-x. Online ahead of print. Cardiovasc Eng Technol. 2025. PMID: 40670735
-
Assessment of arrhythmia mechanism and burden of the infarcted ventricles following remuscularization with pluripotent stem cell-derived cardiomyocyte patches using patient-derived models.Cardiovasc Res. 2022 Mar 25;118(5):1247-1261. doi: 10.1093/cvr/cvab140. Cardiovasc Res. 2022. PMID: 33881518 Free PMC article.
-
Critical Requirements for the Initiation of a Cardiac Arrhythmia in Rat Ventricle: How Many Myocytes?Cells. 2022 Jun 9;11(12):1878. doi: 10.3390/cells11121878. Cells. 2022. PMID: 35741007 Free PMC article.
References
-
- Murray CJ, et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990-2013: quantifying the epidemiological transition. Lancet. 2015;386:2145–2191. doi: 10.1016/S0140-6736(15)61340-X. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
