

Gabapentin in Mixed Drug Fatalities: Does this Frequent Analyte Deserve More Attention?
- PMID: 31239962
- PMCID: PMC6474478
- DOI: 10.23907/2017.012
Gabapentin in Mixed Drug Fatalities: Does this Frequent Analyte Deserve More Attention?
Abstract
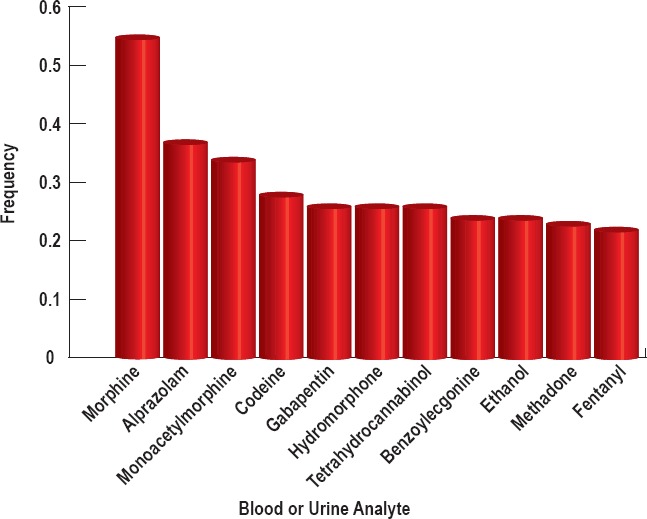
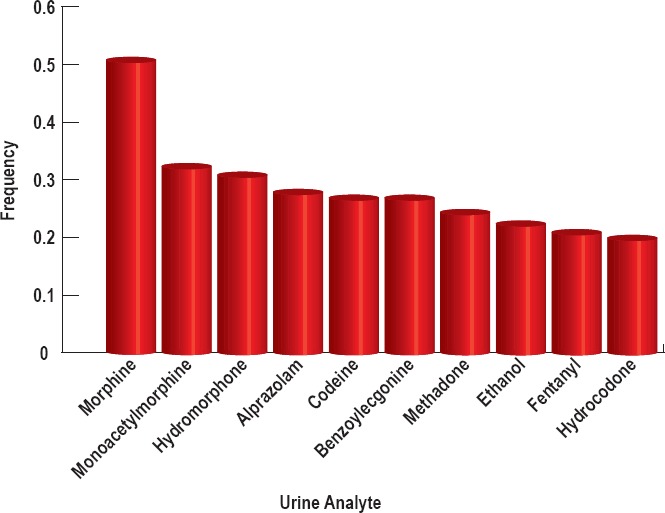
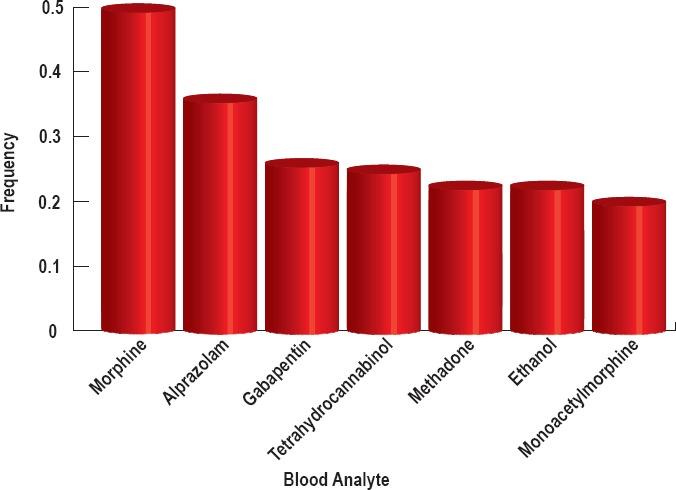
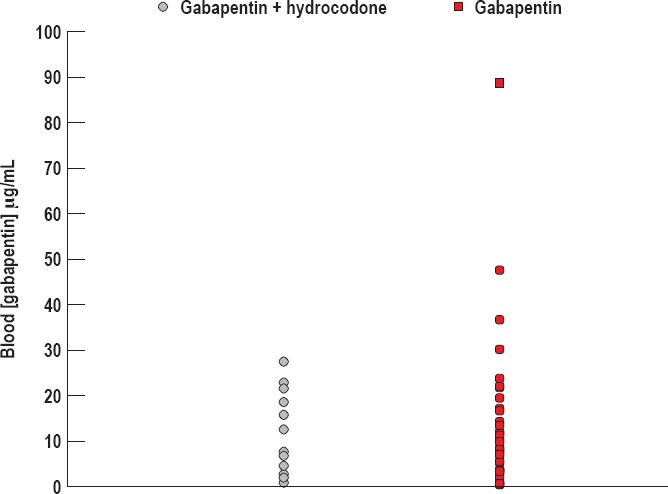
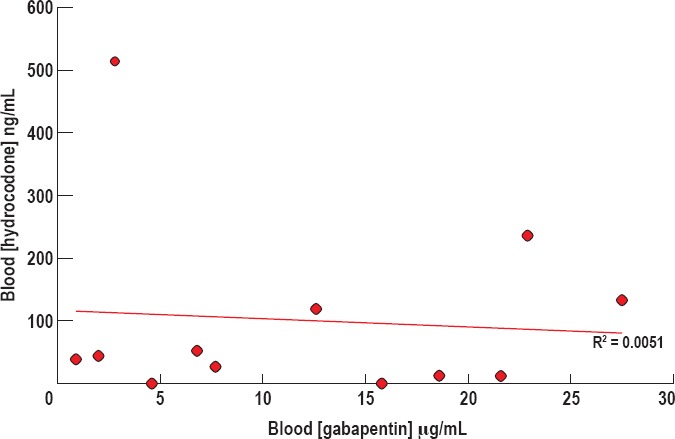
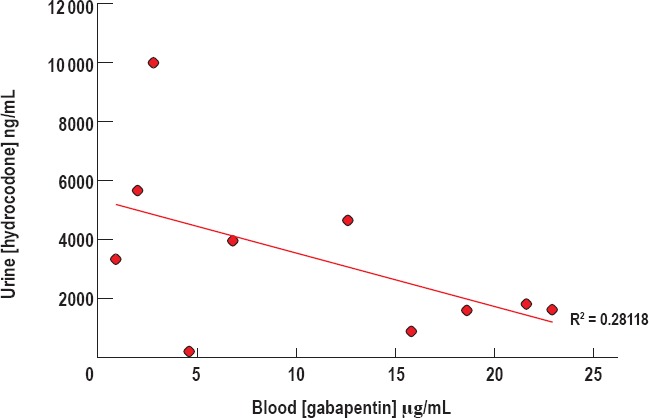
From 2000 to 2014, drug overdose deaths increased 137% in the United States, and 61% of these deaths included some form of opiate. The vast majority of opiate-related drug fatalities include multiple drugs, although there is scant data quantitatively describing the exact drugs that contribute to deaths due to multiple drugs. In the present study, we sought to quantitatively identify the drugs that occur with opiates in accidental multidrug-related fatalities. We retrospectively explored fatal drug trends in four Michigan counties, with a focus on profiling drugs present concurrently with opiates. Blood and urine toxicology reports for mixed drug fatalities (N=180) were analyzed using frequent item analysis approaches to identify common analyte trends in opiate-related fatalities. Within our cohort, the most prevalent serum analytes included caffeine (n=147), morphine (n=90), alprazolam (n=69), gabapentin (n=46), and tetrahydrocannabinol (n=44). In 100% of cases where gabapentin was present (n=46), an opiate was also present in the serum or urine. The average gabapentin serum concentration was 13.56 μg/mL (SEM =0.33 μg/mL), with a range of 0.5-88.7 μg/mL. Gabapentin was found at very high frequency in accidental mixed drug fatalities. Gabapentin concentrations were generally within the normal therapeutic range (2-20 μg/mL). It is unknown whether a synergistic effect with opioids may contribute to central respiratory depression. Further research is warranted to determine any contributory role of gabapentin in these deaths. Confirmed interactions could have broad implications for future reporting by forensic pathologists as well as prescribing practices by clinicians.
Keywords: Forensic pathology; Gabapentin; Hydrocodone; Mixed-drug fatality; Opioid overdose; Substance abuse.
Conflict of interest statement
DISCLOSURES & DECLARATION OF CONFLICTS OF INTEREST The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest
Figures
References
-
- Hahsler M., Grün B., Hornik K., Buchta C. Introduction to arules – a computational environment for mining association rules and frequent item sets. J Stat Softw [Internet]. 2005. [cited 2016 Oct 10]; 14(15): 1–25. Available from: https://cran.r-project.org/web/packages/arules/vignettes/arules.pdf.
LinkOut - more resources
Full Text Sources