

Implementation of a nurse-led protocol for early extubation after cardiac surgery: A pilot study
- PMID: 31240173
- PMCID: PMC6582226
- DOI: 10.5492/wjccm.v8.i3.28
Implementation of a nurse-led protocol for early extubation after cardiac surgery: A pilot study
Abstract
Background: Protocols for nurse-led extubation are as safe as a physician-guided weaning in general intensive care unit (ICU). Early extubation is a cornerstone of fast-track cardiac surgery, and it has been mainly implemented in post-anaesthesia care units. Introducing a nurse-led extubation protocol may lead to reduced extubation time.
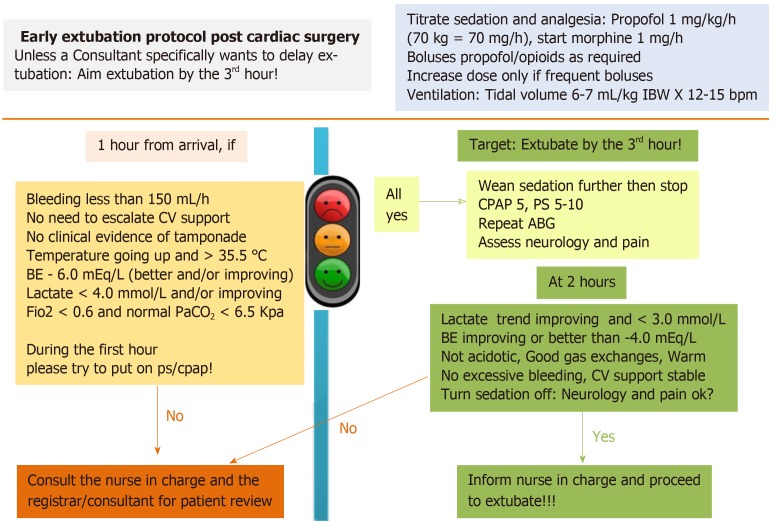
Aim: To investigate results of the implementation of a nurse-led protocol for early extubation after elective cardiac surgery, aiming at higher extubation rates by the third postoperative hour.
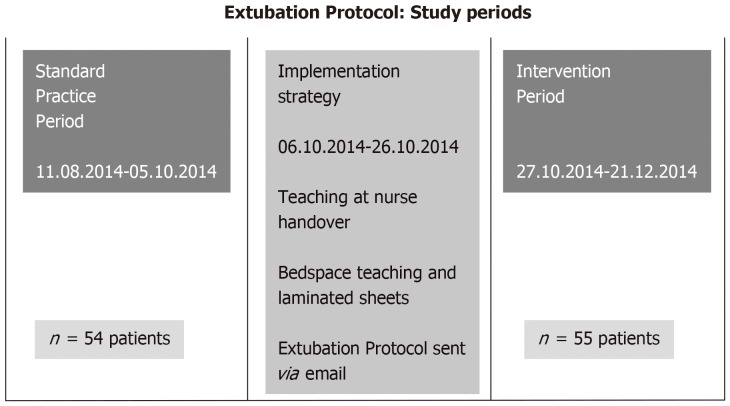
Methods: A single centre prospective study in an 18-bed, consultant-led Cardiothoracic ICU, with a 1:1 nurse-to-patient ratio. During a 3-wk period, the protocol was implemented with: (1) Structured teaching sessions at nurse handover and at bed-space (all staff received teaching, over 90% were exposed at least twice; (2) Email; and (3) Laminated sheets at bed-space. We compared "standard practice" and "intervention" periods before and after the protocol implementation, measuring extubation rates at several time-points from the third until the 24th postoperative hour.
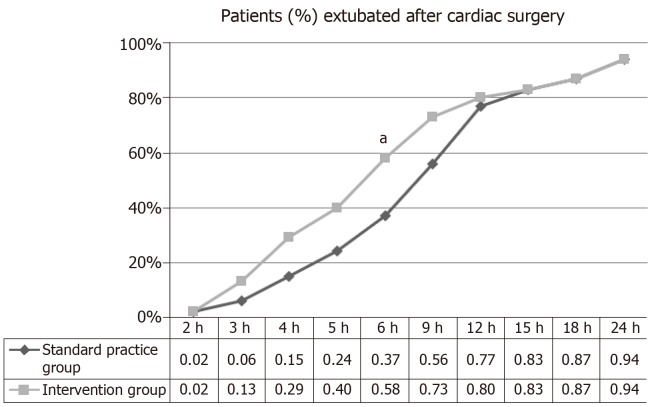
Results: Of 122 cardiac surgery patients admitted to ICU, 13 were excluded as early weaning was considered unsafe. Therefore, 109 patients were included, 54 in the standard and 55 in the intervention period. Types of surgical interventions and baseline left ventricular function were similar between groups. From the third to the 12th post-operative hour, the intervention group displayed a higher proportion of patients extubated compared to the standard group. However, results were significant only at the sixth hour (58% vs 37%, P = 0.04), and not different at the third hour (13% vs 6%, P = 0.33). From the 12th post-operative hour time-point onward, extubation rates became almost identical between groups (83% in standard vs 83% in intervention period).
Conclusion: The implementation of a nurse-led protocol for early extubation after cardiac surgery in ICU may gradually lead to higher rates of early extubation.
Keywords: Extubation protocol; Fast-track; Implementation strategies; Intensive care; Mechanical ventilation.
Conflict of interest statement
Conflict-of-interest statement: Authors declared no conflict-of-interest.
Figures
References
-
- Cheng DC. Fast track cardiac surgery pathways: early extubation, process of care, and cost containment. Anesthesiology. 1998;88:1429–1433. - PubMed
-
- Cheng DC, Karski J, Peniston C, Asokumar B, Raveendran G, Carroll J, Nierenberg H, Roger S, Mickle D, Tong J, Zelovitsky J, David T, Sandler A. Morbidity outcome in early vs conventional tracheal extubation after coronary artery bypass grafting: a prospective randomized controlled trial. J Thorac Cardiovasc Surg. 1996;112:755–764. - PubMed
-
- Cheng DC, Wall C, Djaiani G, Peragallo RA, Carroll J, Li C, Naylor D. Randomized assessment of resource use in fast-track cardiac surgery 1-year after hospital discharge. Anesthesiology. 2003;98:651–657. - PubMed
-
- Zhu F, Lee A, Chee YE. Fast-track cardiac care for adult cardiac surgical patients. Cochrane Database Syst Rev. 2012;10:CD003587. - PubMed
-
- Meade MO, Guyatt G, Butler R, Elms B, Hand L, Ingram A, Griffith L. Trials comparing early vs late extubation following cardiovascular surgery. Chest. 2001;120:445S–453S. - PubMed
LinkOut - more resources
Full Text Sources
