

Assessing bone mineralisation in children with chronic kidney disease: what clinical and research tools are available?
- PMID: 31240395
- PMCID: PMC7184042
- DOI: 10.1007/s00467-019-04271-1
Assessing bone mineralisation in children with chronic kidney disease: what clinical and research tools are available?
Abstract
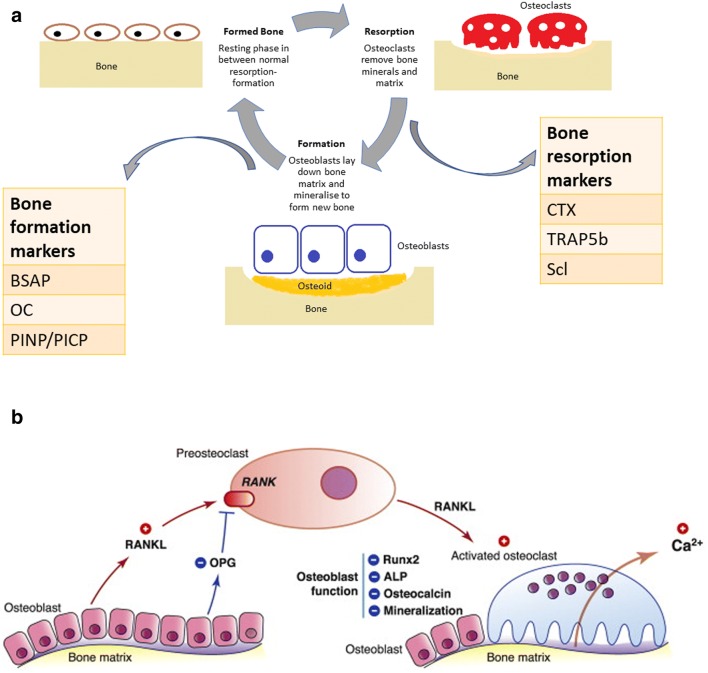
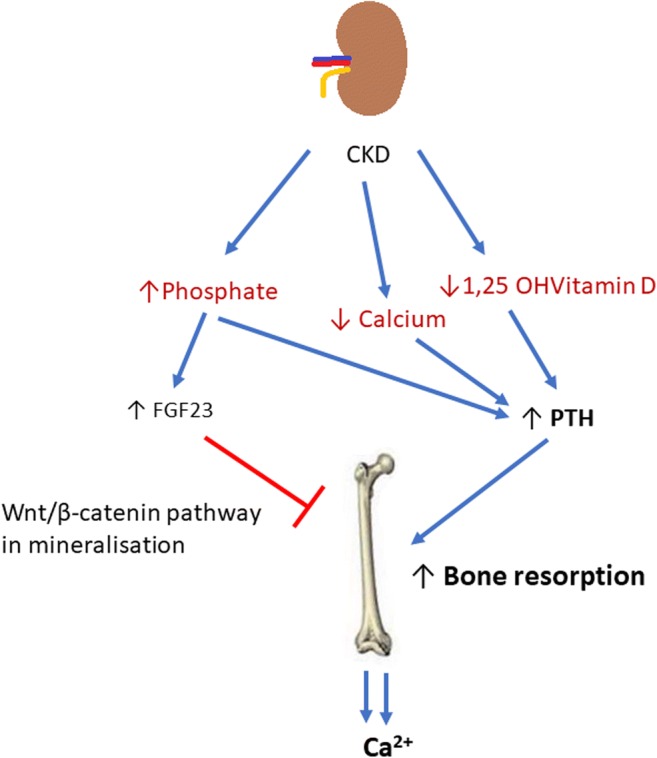
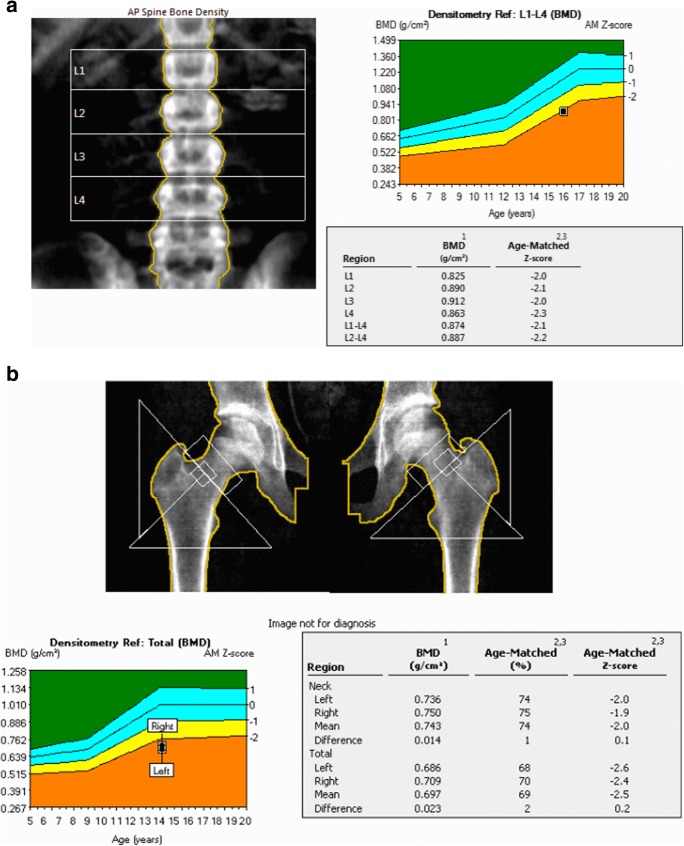
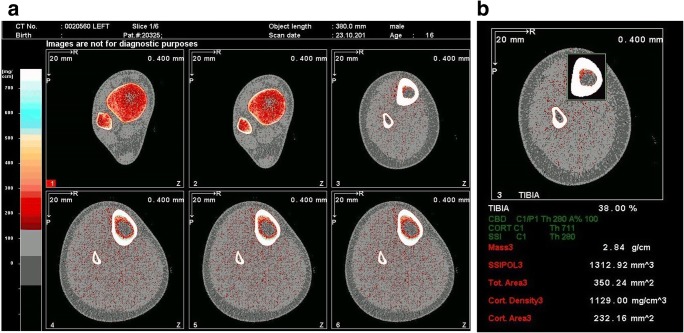
Mineral and bone disorder in chronic kidney disease (CKD-MBD) is a triad of biochemical imbalances of calcium, phosphate, parathyroid hormone and vitamin D, bone abnormalities and soft tissue calcification. Maintaining optimal bone health in children with CKD is important to prevent long-term complications, such as fractures, to optimise growth and possibly also to prevent extra-osseous calcification, especially vascular calcification. In this review, we discuss normal bone mineralisation, the pathophysiology of dysregulated homeostasis leading to mineralisation defects in CKD and its clinical consequences. Bone mineralisation is best assessed on bone histology and histomorphometry, but given the rarity with which this is performed, we present an overview of the tools available to clinicians to assess bone mineral density, including serum biomarkers and imaging such as dual-energy X-ray absorptiometry and peripheral quantitative computed tomography. We discuss key studies that have used these techniques, their advantages and disadvantages in childhood CKD and their relationship to biomarkers and bone histomorphometry. Finally, we present recommendations from relevant guidelines-Kidney Disease Improving Global Outcomes and the International Society of Clinical Densitometry-on the use of imaging, biomarkers and bone biopsy in assessing bone mineral density. Given low-level evidence from most paediatric studies, bone imaging and histology remain largely research tools, and current clinical management is guided by serum calcium, phosphate, PTH, vitamin D and alkaline phosphatase levels only.
Keywords: Bone biopsy; Bone mineralisation; Chronic kidney disease (CKD); Dual-energy X-ray absorptiometry (DXA); Peripheral quantitative CT (pQCT).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Moe S, Drueke T, Cunningham J, Goodman W, Martin K, Olgaard K, Ott S, Sprague S, Lameire N, Eknoyan G. Definition, evaluation, and classification of renal osteodystrophy: a position statement from kidney disease: improving global outcomes (KDIGO) Kidney Int. 2006;69:1945–1953. - PubMed
-
- Ketteler M, Block GA, Evenepoel P, Fukagawa M, Herzog CA, McCann L, Moe SM, Shroff R, Tonelli MA, Toussaint ND, Vervloet MG, Leonard MB. Diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder: synopsis of the kidney disease: improving global outcomes 2017 clinical practice guideline update. Ann Intern Med. 2018;168:422–430. - PubMed
-
- Ketteler M, Block GA, Evenepoel P, Fukagawa M, Herzog CA, McCann L, Moe SM, Shroff R, Tonelli MA, Toussaint ND, Vervloet MG, Leonard MB Executive summary of the 2017 KDIGO chronic kidney disease–mineral and bone disorder (CKD-MBD) guideline update: what’s changed and why it matters. Kidney Int 92:26–36 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
