

Outcomes After Inguinal Hernia Repair With Mesh Performed by Medical Doctors and Surgeons in Ghana
- PMID: 31241736
- PMCID: PMC6596328
- DOI: 10.1001/jamasurg.2019.1744
Outcomes After Inguinal Hernia Repair With Mesh Performed by Medical Doctors and Surgeons in Ghana
Abstract
Importance: Inguinal hernia is the most common general surgical condition in the world. Although task sharing of surgical care with nonsurgeons represents one method to increase access to essential surgery, the safety and outcomes of this strategy are not well described for hernia repair.
Objective: To compare outcomes after inguinal hernia repair with mesh performed by medical doctors and surgeons in Ghana.
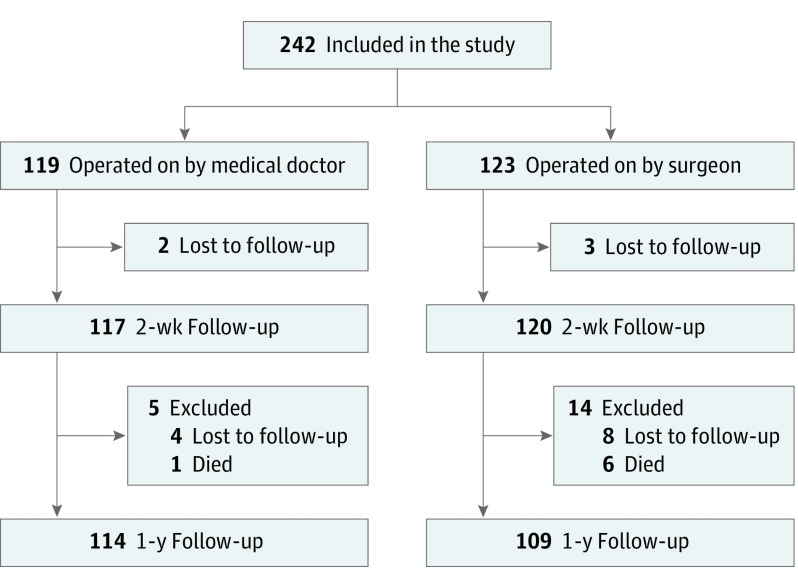
Design, setting, and participants: This prospective cohort study was conducted from February 15, 2017, to September 17, 2018, at the Volta Regional Hospital in Ho, Ghana. Following successful completion of a training course, 3 medical doctors and 2 surgeons performed inguinal hernia repair with mesh according to the Lichtenstein technique on 242 men with primary, reducible inguinal hernia.
Main outcomes and measures: The primary end point was hernia recurrence at 1 year. The noninferiority limit was set at 5 percentage points. Secondary end points included postoperative complications at 2 weeks and patient satisfaction, pain, and self-assessed health status at 1 year.
Results: Two-hundred forty-two patients were included; 119 men underwent operations performed by medical doctors and 123 men underwent operations performed by surgeons. Preoperative patient characteristics were similar in both groups. Two-hundred thirty-seven patients (97.9%) were seen at follow-up at 2 weeks, and 223 patients (92.1%) were seen at follow-up at 1 year. The absolute difference in recurrence rate between the medical doctor group (1 [0.9%]) and the surgeon group (3 [2.8%]) was -1.9 (1-tailed 95% CI, -4.8; P < .001), demonstrating noninferiority of the medical doctors. There were no statistically significant differences in postoperative complications (34 [29.1%] vs 29 [24.2%]), patient satisfaction (112 [98.2%] vs 108 [99.1%]), severe chronic pain (1 [0.9%] vs 4 [3.7%]), or self-assessed health (85.9 vs 83.7 of 100) for medical doctors and surgeons.
Conclusions and relevance: This study shows that medical doctors can be trained to perform elective inguinal hernia repair with mesh in men with good results and high patient satisfaction in a low-resource setting. This finding supports surgical task sharing to combat the global burden of hernia disease.
Conflict of interest statement
Figures
Comment in
-
Task Shifting in Surgery-What US Health Care Can Learn From Ghana.JAMA Surg. 2019 Sep 1;154(9):860. doi: 10.1001/jamasurg.2019.1745. JAMA Surg. 2019. PMID: 31241737 No abstract available.
-
The Realities of External Validity in Global Surgery Research-Reply.JAMA Surg. 2020 Feb 1;155(2):172-173. doi: 10.1001/jamasurg.2019.4090. JAMA Surg. 2020. PMID: 31642875 No abstract available.
-
International Consensus and External Validity in Global Surgery Research and Task Shifting-Reply.JAMA Surg. 2020 Feb 1;155(2):171-172. doi: 10.1001/jamasurg.2019.4088. JAMA Surg. 2020. PMID: 31642883 No abstract available.
-
International Consensus and External Validity in Global Surgery Research and Task Shifting.JAMA Surg. 2020 Feb 1;155(2):171. doi: 10.1001/jamasurg.2019.4087. JAMA Surg. 2020. PMID: 31642885 No abstract available.
-
The Realities of External Validity in Global Surgery Research.JAMA Surg. 2020 Feb 1;155(2):172. doi: 10.1001/jamasurg.2019.4089. JAMA Surg. 2020. PMID: 31642887 No abstract available.
Similar articles
-
The State of Surgical Task Sharing for Inguinal Hernia Repair in Limited-Resource Countries.World J Surg. 2020 Jun;44(6):1719-1726. doi: 10.1007/s00268-020-05390-9. World J Surg. 2020. PMID: 32144469 Review.
-
Long-Term Outcomes Following Inguinal Hernia Repair With Mesh Performed by Medical Doctors and Surgeons in Ghana.Ann Surg Open. 2024 Jul 15;5(3):e460. doi: 10.1097/AS9.0000000000000460. eCollection 2024 Sep. Ann Surg Open. 2024. PMID: 39310350 Free PMC article.
-
Outcomes After Elective Inguinal Hernia Repair Performed by Associate Clinicians vs Medical Doctors in Sierra Leone: A Randomized Clinical Trial.JAMA Netw Open. 2021 Jan 4;4(1):e2032681. doi: 10.1001/jamanetworkopen.2020.32681. JAMA Netw Open. 2021. PMID: 33427884 Free PMC article. Clinical Trial.
-
Explaining variation in ventral and inguinal hernia repair outcomes: A population-based analysis.Surgery. 2017 Sep;162(3):628-639. doi: 10.1016/j.surg.2017.03.013. Epub 2017 May 18. Surgery. 2017. PMID: 28528663
-
Lightweight mesh is recommended in open inguinal (Lichtenstein) hernia repair: A systematic review and meta-analysis.Surgery. 2020 Mar;167(3):581-589. doi: 10.1016/j.surg.2019.08.021. Epub 2019 Oct 28. Surgery. 2020. PMID: 31672519
Cited by
-
An international survey of 1014 hernia surgeons: outcome of GLACIER (global practice of inguinal hernia repair) study.Hernia. 2023 Oct;27(5):1235-1243. doi: 10.1007/s10029-023-02818-8. Epub 2023 Jun 13. Hernia. 2023. PMID: 37310493
-
Economic evaluation of expanding inguinal hernia repair among adult males in Sierra Leone.PLOS Glob Public Health. 2024 Dec 12;4(12):e0003861. doi: 10.1371/journal.pgph.0003861. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 39666633 Free PMC article.
-
Rare but important gastrointestinal complications after laparoscopic inguinal hernia repair: a single-center experience.Sci Rep. 2025 Jan 21;15(1):2593. doi: 10.1038/s41598-025-87188-0. Sci Rep. 2025. PMID: 39833488 Free PMC article.
-
Task Shifting and Task Sharing to Strengthen the Surgical Workforce in Sub-Saharan Africa: A Systematic Review of the Existing Literature.World J Surg. 2023 Dec;47(12):3070-3080. doi: 10.1007/s00268-023-07197-w. Epub 2023 Oct 13. World J Surg. 2023. PMID: 37831136
-
The State of Surgical Task Sharing for Inguinal Hernia Repair in Limited-Resource Countries.World J Surg. 2020 Jun;44(6):1719-1726. doi: 10.1007/s00268-020-05390-9. World J Surg. 2020. PMID: 32144469 Review.
References
-
- Beard JH, Ohene-Yeboah M, Devries CR, Schecter WP. Hernia and hydrocele In: Debas HT, Donkor P, Gawande A, Jamison DT, Kruk ME, Mock CN, eds. Essential Surgery: Disease Control Priorities, Third Edition (Volume 1). Washington, DC: International Bank for Reconstruction and Development, World Bank; 2015:chap 9. - PubMed
