

Estimation of microvascular perfusion after esophagectomy: a quantitative model of dynamic fluorescence imaging
- PMID: 31243624
- PMCID: PMC6706368
- DOI: 10.1007/s11517-019-01994-z
Estimation of microvascular perfusion after esophagectomy: a quantitative model of dynamic fluorescence imaging
Abstract
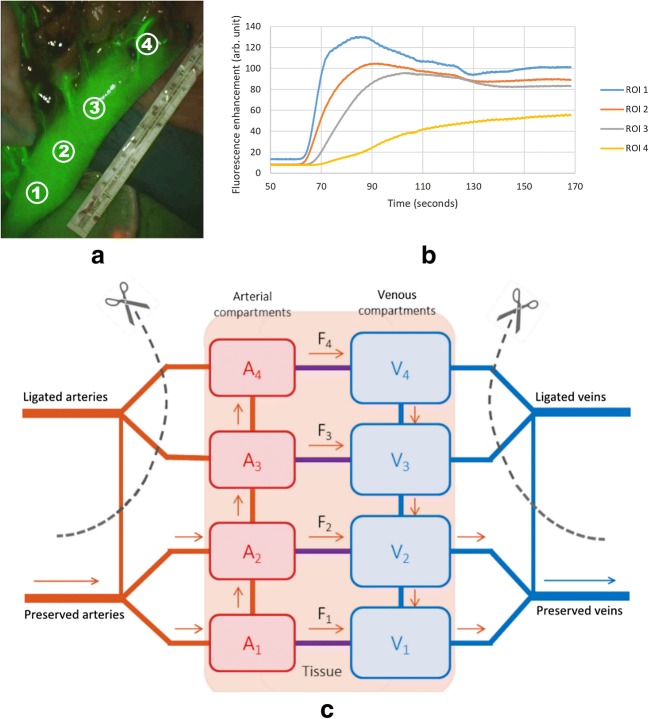
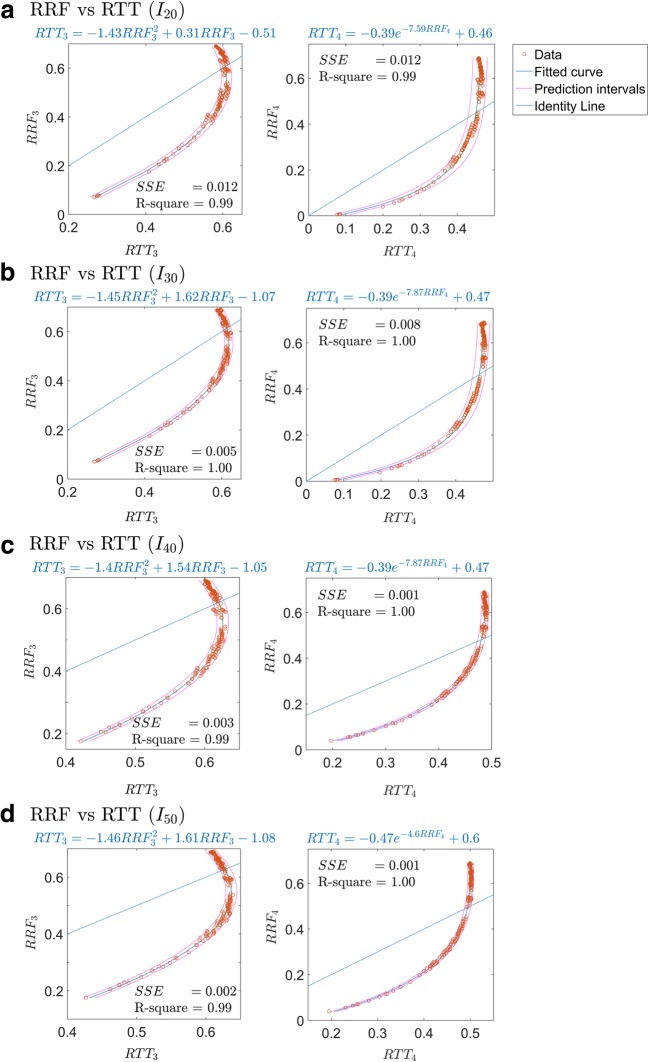
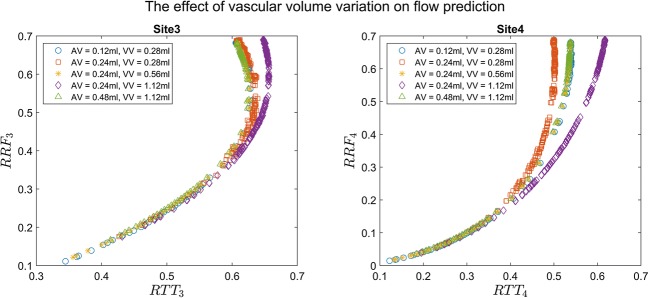
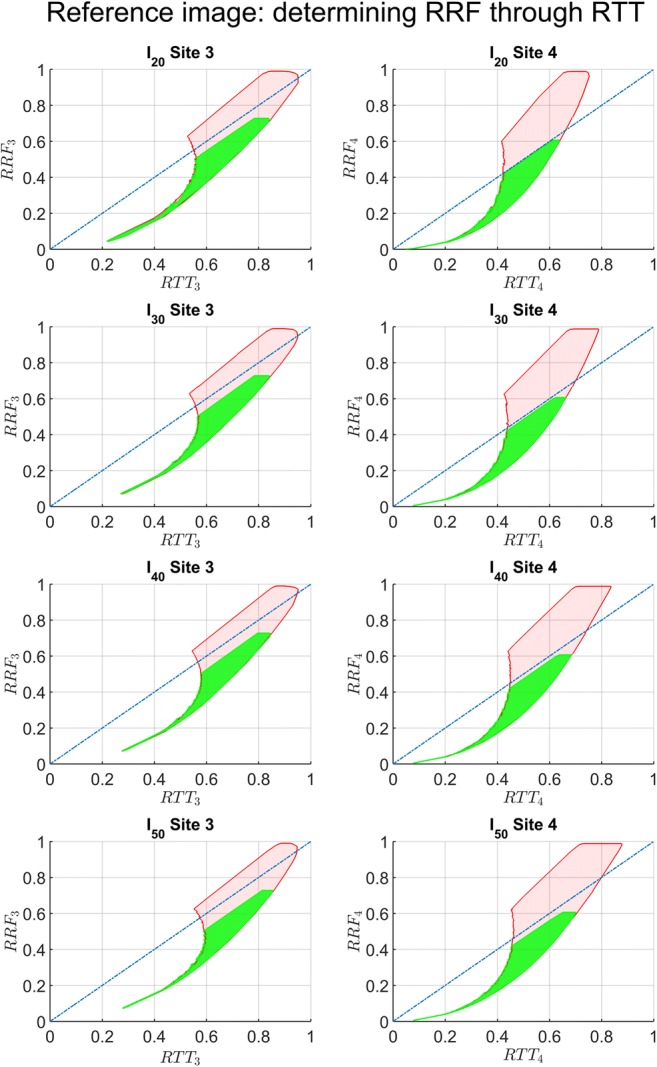
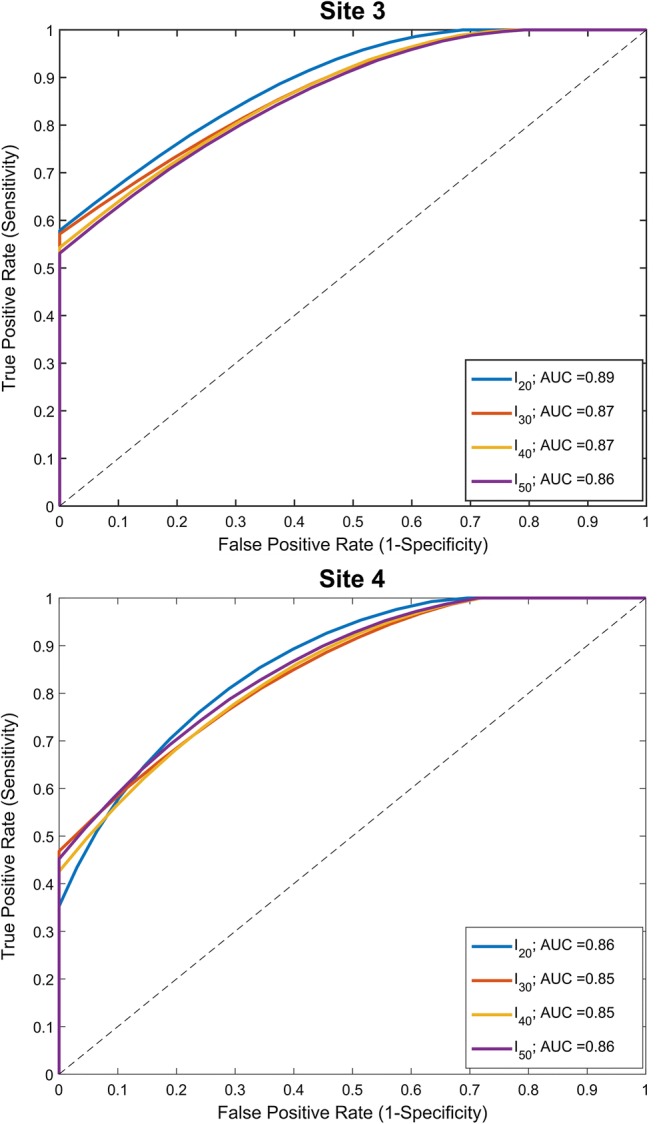
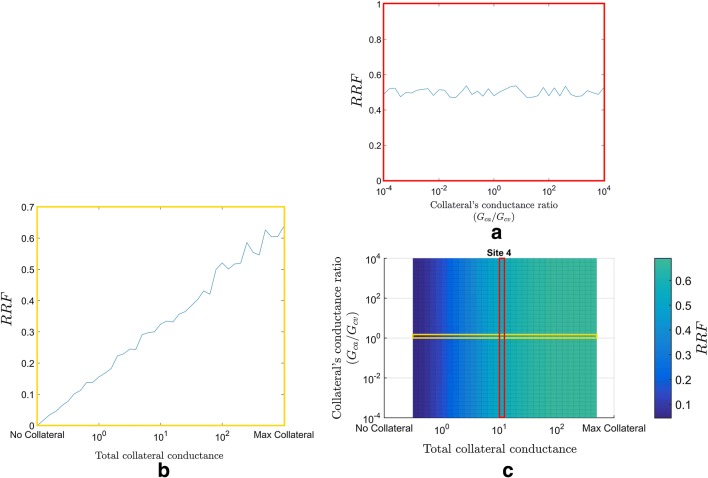
Most common complications of esophagectomy stem from a perfusion deficiency of the gastric conduit at the anastomosis. Fluorescent tracer imaging allows intraoperative visualization of tissue perfusion. Quantitative assessment of fluorescence dynamics has the potential to identify perfusion deficiency. We developed a perfusion model to analyze the relation between fluorescence dynamics and perfusion deficiency. The model divides the gastric conduit into two well-perfused and two anastomosed sites. Hemodynamics and tracer transport were modeled. We analyzed the value of relative time-to-threshold (RTT) as a predictor of the relative remaining flow (RRF). Intensity thresholds for RTT of 20% to 50% of the maximum fluorescence intensity of the well-perfused site were tested. The relation between RTT and RRF at the anastomosed sites was evaluated over large variations of vascular conductance and volume. The ability of RTT to distinguish between sufficient and impaired perfusion was analyzed using c-statistics. We found that RTT was a valuable estimate for low RRF. The threshold of 20% of the maximum fluorescence intensity provided the best prediction of impaired perfusion on the two anastomosed sites (AUC = 0.89 and 0.86). The presented model showed that for low flows, relative time-to-threshold may be used to estimate perfusion deficiency.
Keywords: Esophagectomy; Fluorescence imaging; Gastric conduit model; Indocyanine green; Perfusion.
Conflict of interest statement
Henk A. Marquering is a co-founder and shareholder of Nico.lab. Ton G. van Leeuwen reports grants from ZonMW. Suzanne S. Gisbertz reports a consultancy agreement with Medtronic and grants from Olympus outside the submitted work. The other authors declare that they have no conflict of interest.
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
