

Rare case of an upper urinary tract carcinoma (UTUC) in renal pelvis and ureter associated to renal vein thrombosis: diagnostic imaging with CECT, MRI and CEUS
- PMID: 31243704
- PMCID: PMC6704220
- DOI: 10.1007/s40477-019-00396-z
Rare case of an upper urinary tract carcinoma (UTUC) in renal pelvis and ureter associated to renal vein thrombosis: diagnostic imaging with CECT, MRI and CEUS
Erratum in
-
Correction to: Rare case of an upper urinary tract carcinoma (UTUC) in renal pelvis and ureter associated to renal vein thrombosis: diagnostic imaging with CECT, MRI and CEUS.J Ultrasound. 2019 Sep;22(3):371. doi: 10.1007/s40477-019-00397-y. J Ultrasound. 2019. PMID: 31317338 Free PMC article.
Abstract
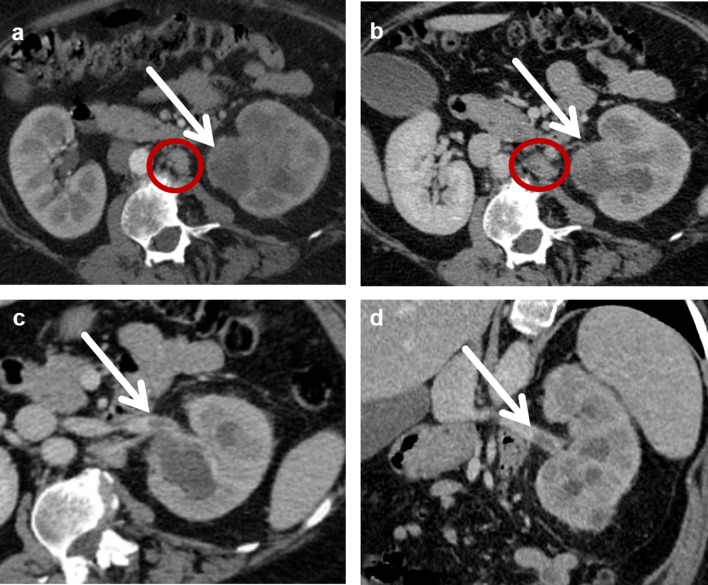
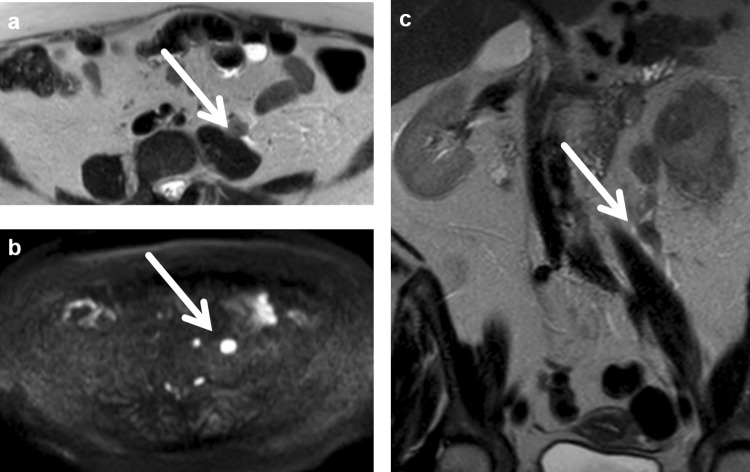
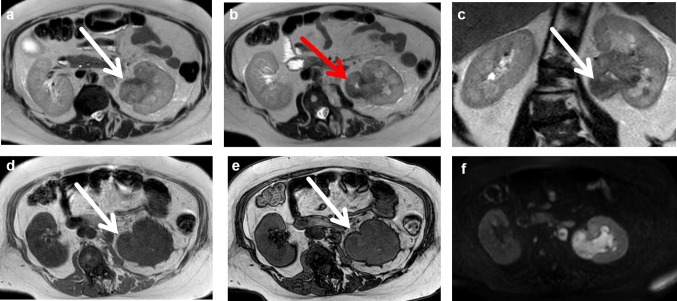
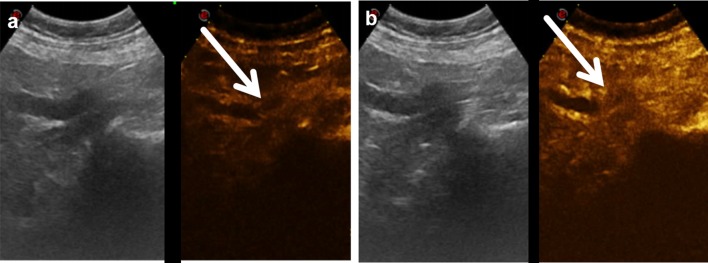
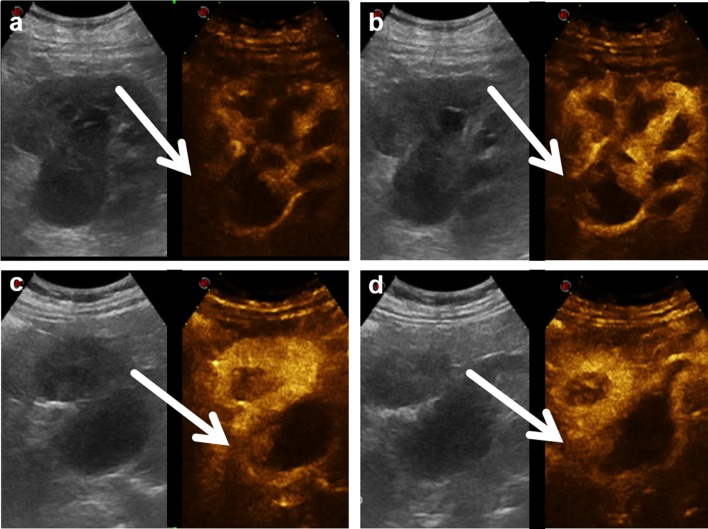
A 58-year-old woman complaining of dyspnea and mild flank pain was admitted to our radiology department after undergoing ultrasonography in another institution. She showed hydronephrosis and left kidney swelling. We performed a contrast-enhanced computed tomography (CECT) that confirmed the hydronephrosis and revealed a widely hypoperfused left kidney, a concentric thickening of the proximal ureter, and a slight and diffuse thickening of the renal pelvic wall, with a hyperdense content in the unenhanced CT phase and poor contrast enhancement in the post-contrast phases. A proximal ipsilateral renal vein thrombosis was associated. Non-contrast magnetic resonance imaging confirmed the CECT findings. At the same time, we performed a contrast-enhanced ultrasonography examination, which proved to be helpful for the characterization of the lesion and for patient management.
Keywords: Contrast-enhanced computed tomography; Contrast-enhanced ultrasonography; Magnetic resonance imaging; Renal vein thrombosis; Urothelial carcinoma.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
