

Clinicopathologic correlations in a family with a TBK1 mutation presenting as primary progressive aphasia and primary lateral sclerosis
- PMID: 31244341
- PMCID: PMC6768716
- DOI: 10.1080/21678421.2019.1632347
Clinicopathologic correlations in a family with a TBK1 mutation presenting as primary progressive aphasia and primary lateral sclerosis
Abstract
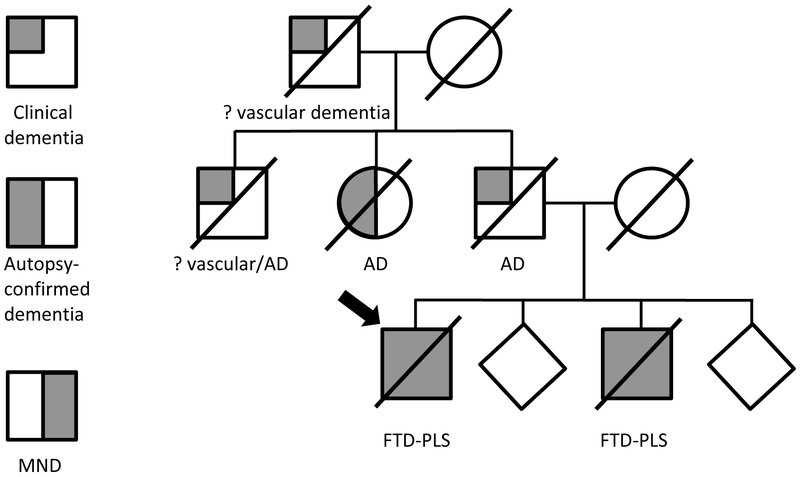
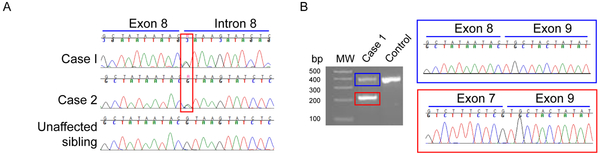
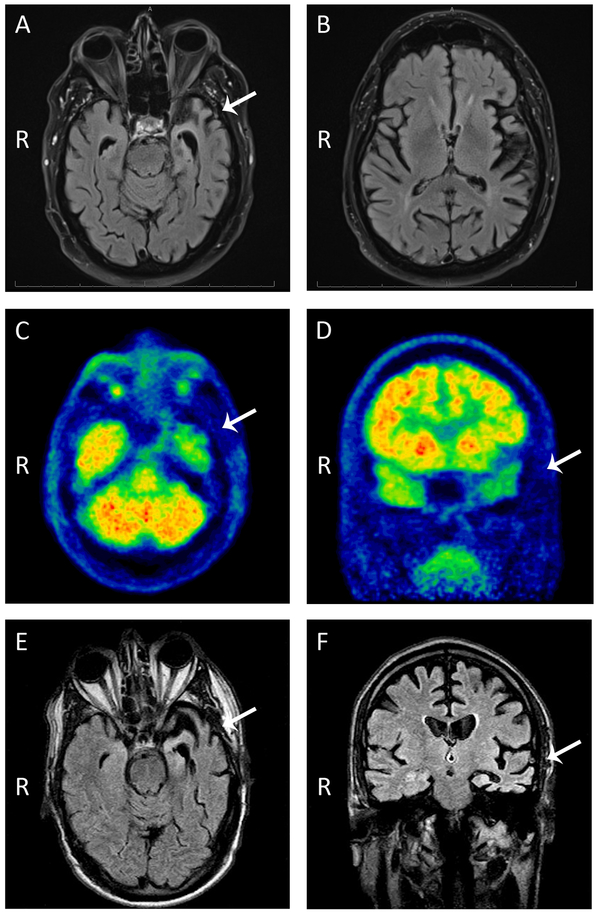
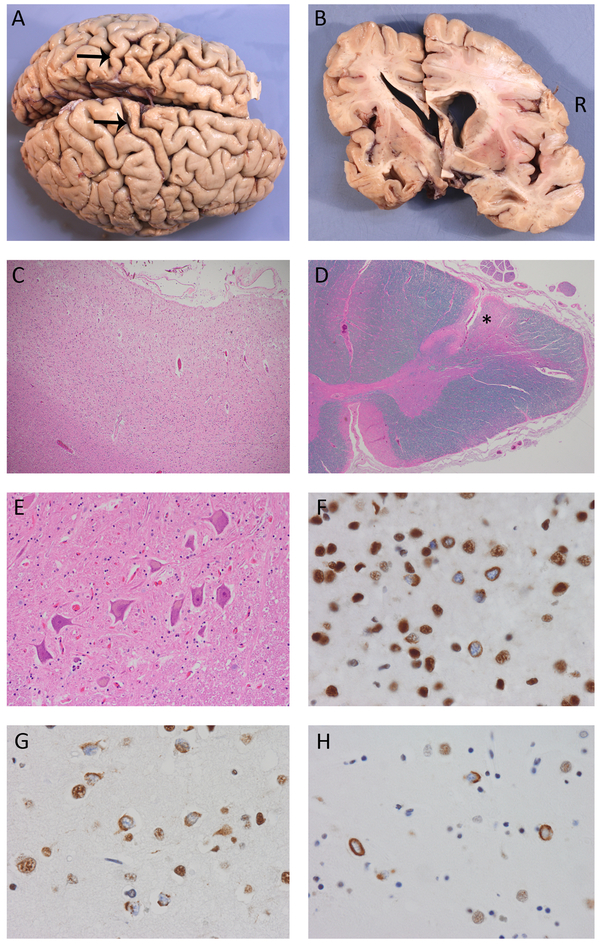
Mutations in the TANK binding kinase 1 gene (TBK1) are associated with amyotrophic lateral sclerosis and/or frontotemporal dementia; however, the range of clinical phenotypes and neuropathological changes associated with these mutations have not yet been completely elucidated. We present the detailed clinical, neuroimaging, and neuropathological features of two brothers carrying the TBK1 p.Gly272_Thr331del mutation. Both presented with very similar and unusual clinical features including primary progressive aphasia and asymmetric-onset primary lateral sclerosis (PLS). Repeated electrophysiological studies failed to reveal any lower motor neuron involvement. Neuropathological evaluation of both cases revealed frontotemporal lobar degeneration with TDP-43 proteinopathy type B and selective involvement of upper motor neurons with TDP-43 inclusions. The stereotypical clinical presentation and neuropathological findings in these cases widen the phenotypic spectrum of TBK1 mutations and provide insights into the pathogenesis of PLS.
Keywords: TBK1; TDP-43; neuropathology; primary lateral sclerosis; primary progressive aphasia.
Conflict of interest statement
Declaration of interest statement
None of the authors has conflicts of interest to declare.
Figures
References
-
- Ringholz GM, Appel SH, Bradshaw M, Cooke NA, Mosnik DM, Schulz PE. Prevalence and patterns of cognitive impairment in sporadic ALS Neurology. Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology; 2005. August 23;65(4):586–90. - PubMed
-
- Lomen-Hoerth C, Murphy J, Langmore S, Kramer JH, Olney RK, Miller B. Are amyotrophic lateral sclerosis patients cognitively normal? Neurology. Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology; 2003. April 8;60(7):1094–7. - PubMed
-
- de Vries BS, Rustemeijer LMM, van der Kooi AJ, Raaphorst J, Schröder CD, Nijboer TCW, et al. A case series of PLS patients with frontotemporal dementia and overview of the literature Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration. Taylor & Francis; 2017. November;18(7-8):534–48. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous