

The irreversible HCV-associated risk of gastric cancer following interferon-based therapy: a joint study of hospital-based cases and nationwide population-based cohorts
- PMID: 31244896
- PMCID: PMC6582290
- DOI: 10.1177/1756284819855732
The irreversible HCV-associated risk of gastric cancer following interferon-based therapy: a joint study of hospital-based cases and nationwide population-based cohorts
Abstract
Background: Hepatitis C virus (HCV) infection causes many extrahepatic malignancies; whether it increases gastric cancer risk and the risk reverses after anti-HCV therapy remain elusive.
Method: A nationwide population-based cohort study of Taiwan National Health Insurance Research Database (TNHIRD) was conducted. In parallel, the risk factors and HCV-core-protein expressions were surveyed in gastric cancer patients from a tertiary care center.
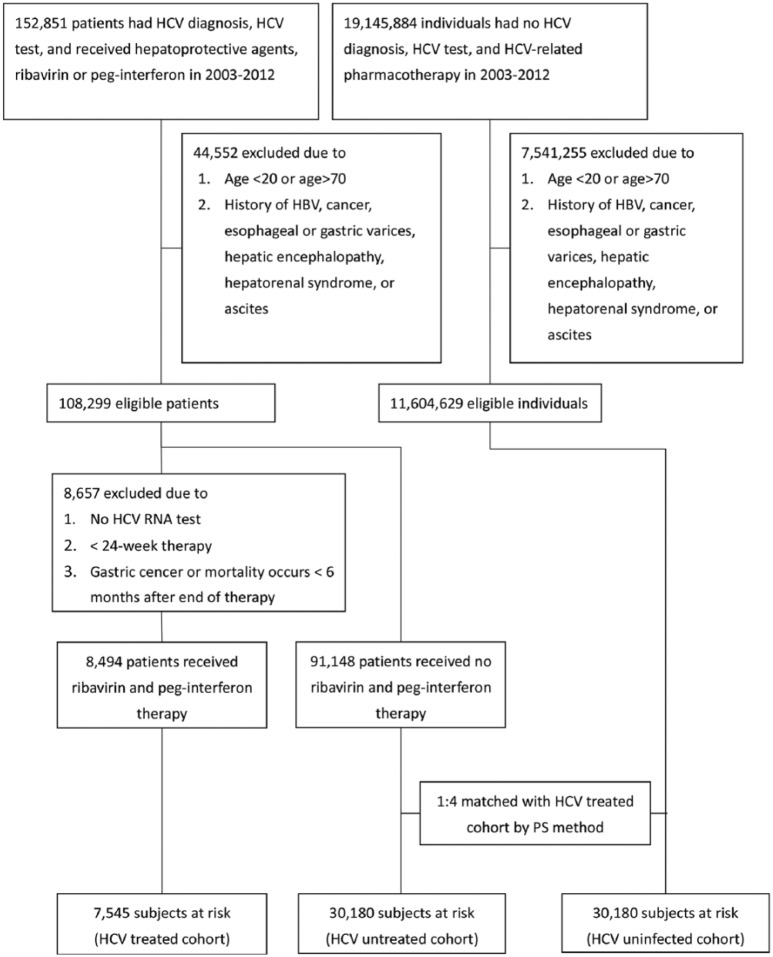
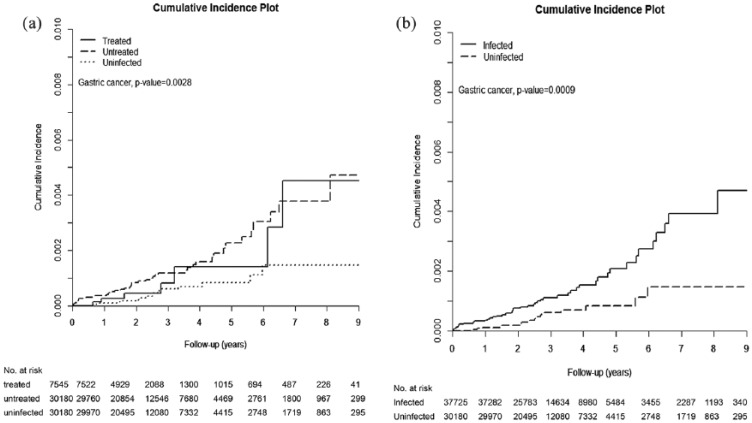
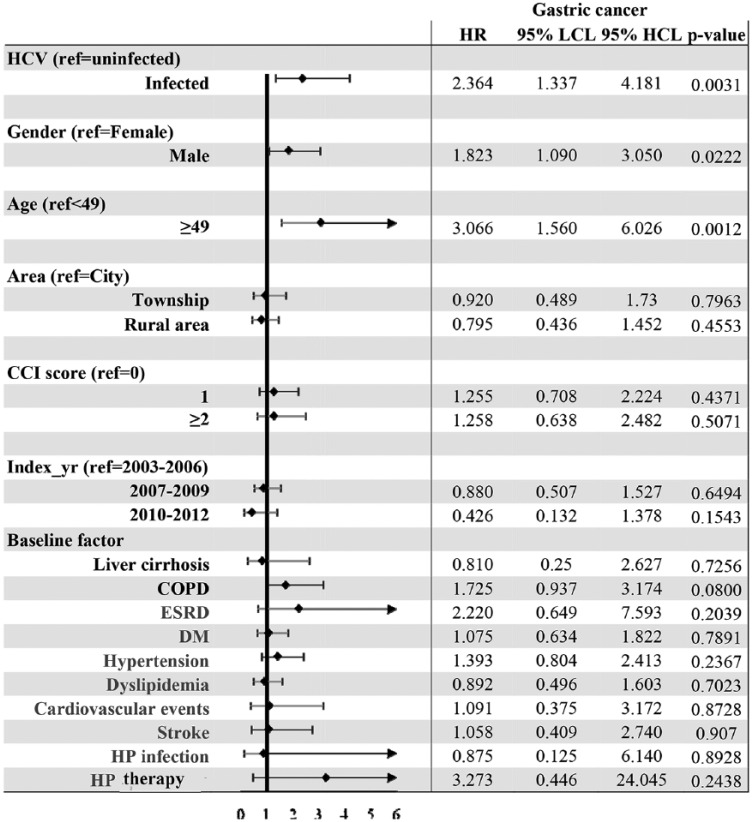
Results: From 2003 to 2012, of 11,712,928 patients, three 1:4:4, propensity-score-matched TNHIRD cohorts including HCV-treated (7545 patients with interferon-based therapy ⩾ 6 months), HCV-untreated (n = 30,180), and HCV-uninfected cohorts (n = 30,180) were enrolled. The cumulative incidences of gastric cancer [HCV-treated: 0.452%; 95% confidence interval (CI): 0.149-1.136%; HCV-untreated: 0.472%; 95% CI: 0.274-0.776%; HCV-uninfected: 0.146%; 95% CI 0.071-0.280%] were lowest in HCV-uninfected cohort (p = 0.0028), but indifferent between treated and untreated cohorts. HCV infection [hazards ratio (HR): 2.364; 95% CI: 1.337-4.181], male sex (HR: 1.823; 95% CI: 1.09-3.05) and age ⩾ 49 years (HR: 3.066; 95% CI: 1.56-6.026) were associated with incident gastric cancers. Among 887 (males: 68.4%; mean age: 66.5 ± 12.9 years, 2008-2018) hospitalized gastric cancer patients, HCV Ab-positive rate was 7.8%. None of the investigated factors exhibited different rates between HCV Ab-positive and Ab-negative patients. No HCV-core-positive cells were demonstrated in gastric cancer tissues.
Conclusions: HCV infection, male sex and old age were risk factors for gastric cancer development. HCV-associated gastric cancer risk might be neither reversed by interferon-based therapy, nor associated with in situ HCV-core-related carcinogenesis.
Keywords: HCV; age; gastric cancer; sex.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
References
-
- Ramos-Casals M, Stone JH, Cid MC, et al. The cryoglobulinaemias. Lancet 2012; 379: 348–360. - PubMed
-
- Negro F, Forton D, Craxì A, et al. Extrahepatic morbidity and mortality of chronic hepatitis C. Gastroenterology 2015; 149: 1345–1360. - PubMed
-
- Su TH, Liu CJ, Tseng TC, et al. Hepatitis C viral infection increases the risk of lymphoid-neoplasms: a population-based cohort study. Hepatology 2016; 63: 721–730. - PubMed
LinkOut - more resources
Full Text Sources
