

Serious infection risk in rheumatoid arthritis compared with non-inflammatory rheumatic and musculoskeletal diseases: a US national cohort study
- PMID: 31245055
- PMCID: PMC6560658
- DOI: 10.1136/rmdopen-2019-000935
Serious infection risk in rheumatoid arthritis compared with non-inflammatory rheumatic and musculoskeletal diseases: a US national cohort study
Abstract
Objectives: To identify serious infection (SI) risk by aetiology and site in patients with rheumatoid arthritis (RA) compared with those with non-inflammatory rheumatic and musculoskeletal diseases (NIRMD).
Methods: Patients participating in FORWARD from 2001 to 2016 were assessed for SIs; defined by infections requiring hospitalisation, intravenous antibiotics or followed by death. SIs were categorised by aetiology and site. SI risk was assessed through Cox proportional hazards models. Best models were selected using machine learning Least Absolute Shrinkage and Selection Operator (LASSO) methodology.
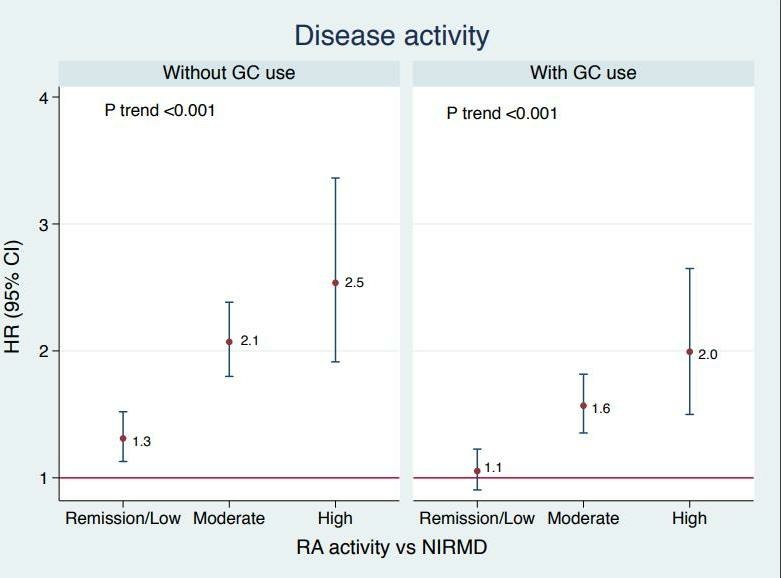
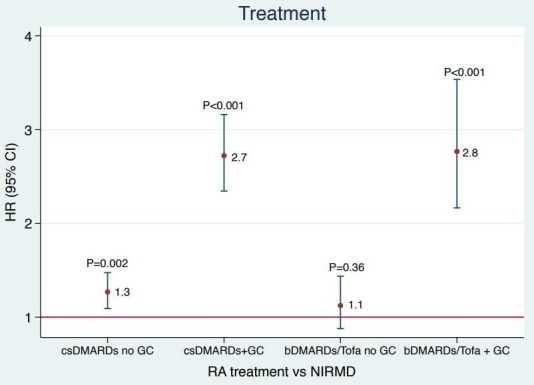
Results: Among 20 361 patients with RA and 6176 patients with NIRMD, 1600 and 276 first SIs were identified, respectively. Incidence of SIs was higher in RA compared with NIRMD (IRR = 1.5; 95% CI 1.2 to 1.5). The risk persisted after adjusting using the LASSO model (HR 1.7; 95% CI 1.5 to 1.8), but attenuated when additionally adjusted for glucocorticoid use (HR 1.3; 95% CI 1.2 to 1.5). SI risk was significantly higher in RA versus NIRMD for bacterial infections as well as for respiratory, skin, bone, joint, bloodstream infections and sepsis irrespective of glucocorticoid use. Compared with NIRMD, SI risk was significantly increased in patients with RA who were in moderate and high disease activity but was similar to those in low disease activity/remission (p trend < 0.001).
Conclusions: The risk of all SIs, particularly bacterial, respiratory, bloodstream, sepsis, skin, bone and joint infections are significantly increased in patients with RA compared with patients with NIRMD. This infection risk appears to be greatest in those with higher RA disease activity.
Keywords: cohort study; non-inflammatory rheumatic disease; rheumatoid arthritis; serious infection.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Björnådal L, Baecklund E, Yin L, et al. Decreasing mortality in patients with rheumatoid arthritis: results from a large population based cohort in Sweden, 1964-95. J Rheumatol 2002;29:906–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical