

Requirements and validation of a prototype learning health system for clinical diagnosis
- PMID: 31245568
- PMCID: PMC6508515
- DOI: 10.1002/lrh2.10026
Requirements and validation of a prototype learning health system for clinical diagnosis
Abstract
Introduction: Diagnostic error is a major threat to patient safety in the context of family practice. The patient safety implications are severe for both patient and clinician. Traditional approaches to diagnostic decision support have lacked broad acceptance for a number of well-documented reasons: poor integration with electronic health records and clinician workflow, static evidence that lacks transparency and trust, and use of proprietary technical standards hindering wider interoperability. The learning health system (LHS) provides a suitable infrastructure for development of a new breed of learning decision support tools. These tools exploit the potential for appropriate use of the growing volumes of aggregated sources of electronic health records.
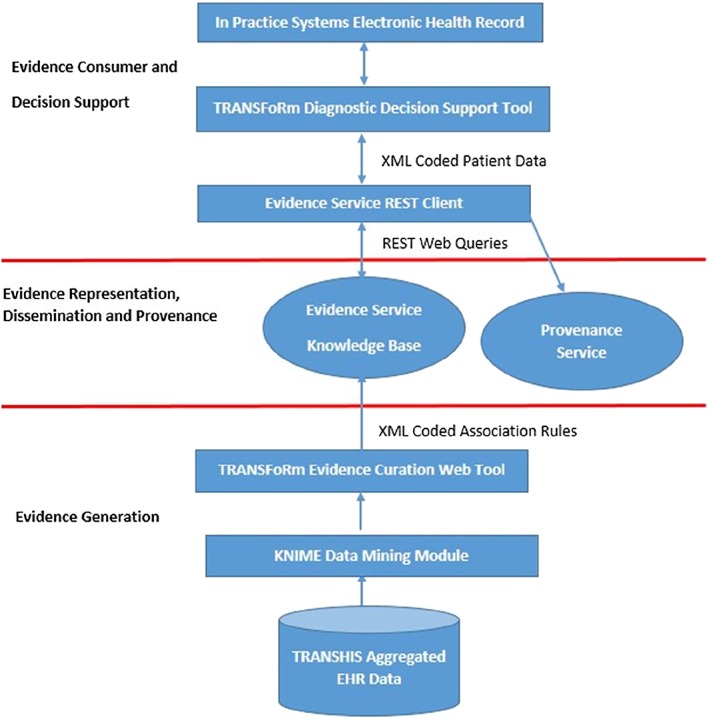
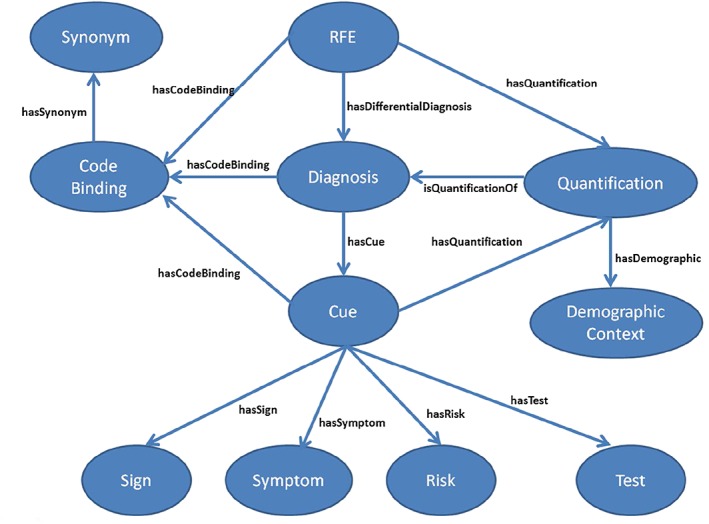
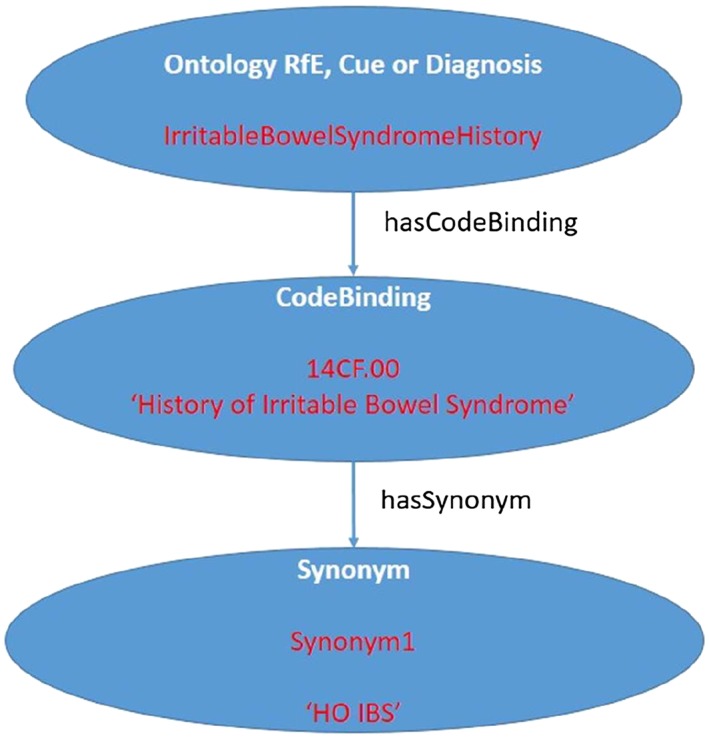
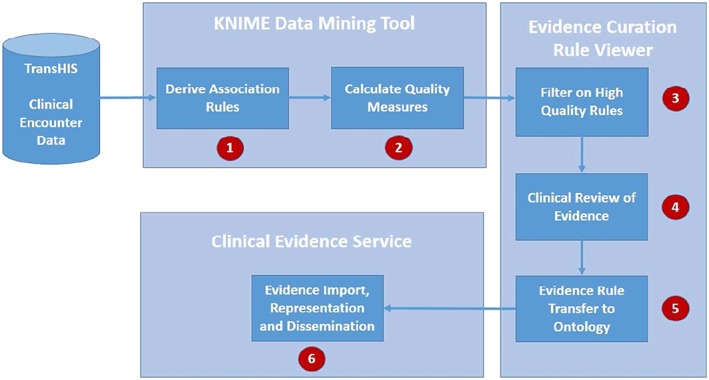
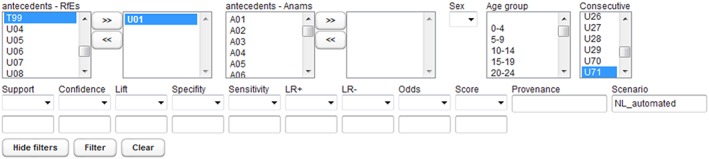
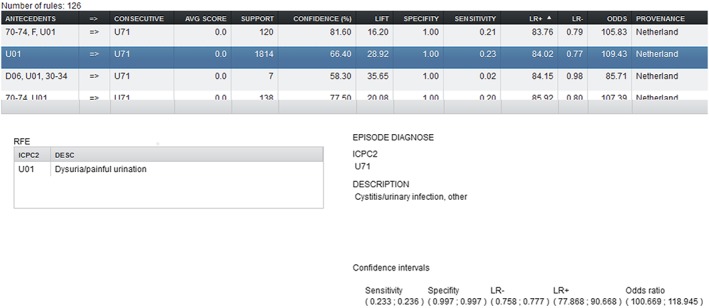
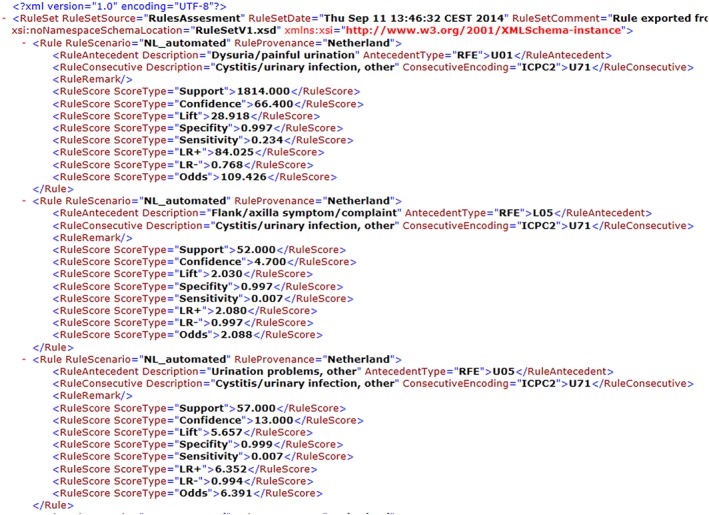
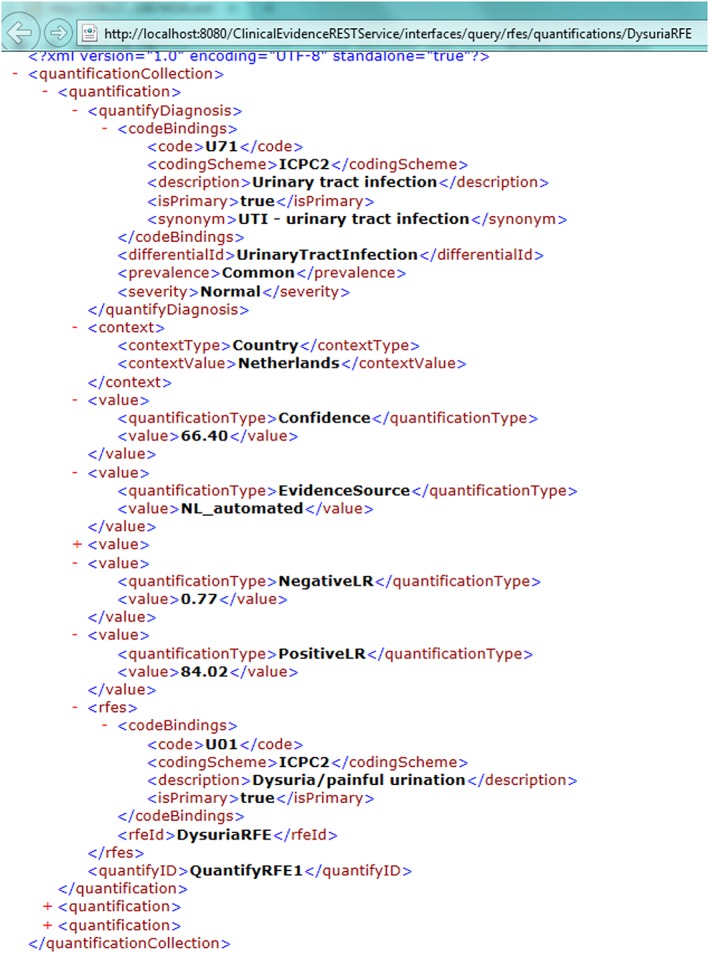
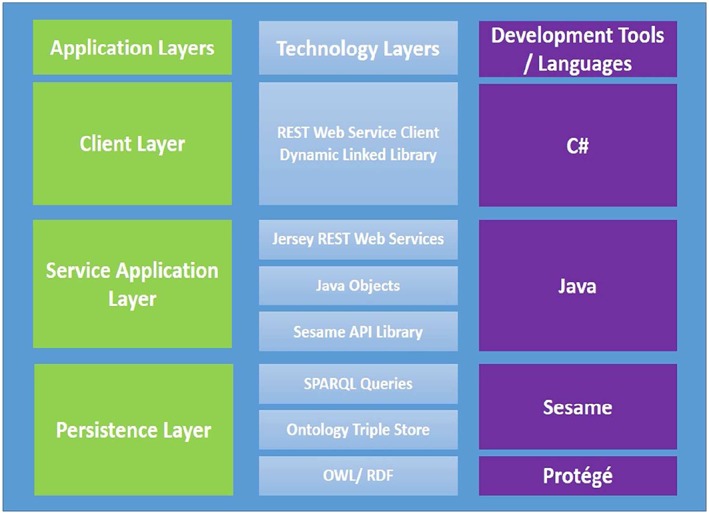
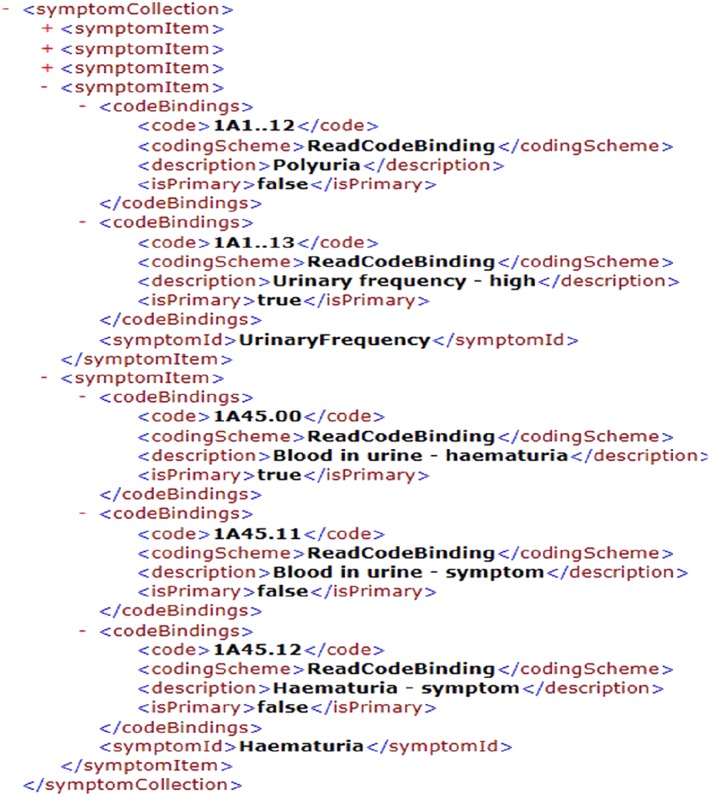
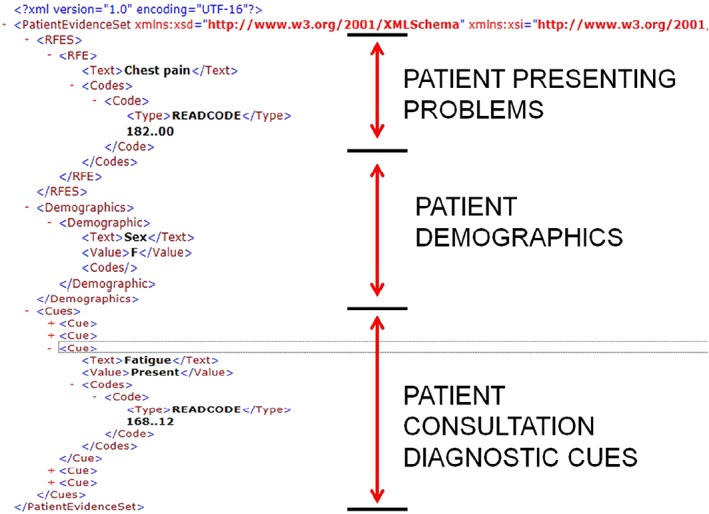
Methods: We describe the experiences of the TRANSFoRm project developing a diagnostic decision support infrastructure consistent with the wider goals of the LHS. We describe an architecture that is model driven, service oriented, constructed using open standards, and supports evidence derived from electronic sources of patient data. We describe the architecture and implementation of 2 critical aspects for a successful LHS: the model representation and translation of clinical evidence into effective practice and the generation of curated clinical evidence that can be used to populate those models, thus closing the LHS loop.
Results/conclusions: Six core design requirements for implementing a diagnostic LHS are identified and successfully implemented as part of this research work. A number of significant technical and policy challenges are identified for the LHS community to consider, and these are discussed in the context of evaluating this work: medico-legal responsibility for generated diagnostic evidence, developing trust in the LHS (particularly important from the perspective of decision support), and constraints imposed by clinical terminologies on evidence generation.
Keywords: diagnostic decision support systems; knowledge discovery; knowledge representation; learning health systems.
Figures
Similar articles
-
Leaders' perspectives on learning health systems: a qualitative study.BMC Health Serv Res. 2020 Nov 26;20(1):1087. doi: 10.1186/s12913-020-05924-w. BMC Health Serv Res. 2020. PMID: 33243214 Free PMC article.
-
The TRANSFoRm project: Experience and lessons learned regarding functional and interoperability requirements to support primary care.Learn Health Syst. 2017 Sep 6;2(2):e10037. doi: 10.1002/lrh2.10037. eCollection 2018 Apr. Learn Health Syst. 2017. PMID: 31245579 Free PMC article.
-
Building a Sustainable Learning Health Care System for Pregnant and Lactating People: Interview Study Among Data Access Providers.JMIR Pediatr Parent. 2024 Feb 8;7:e47092. doi: 10.2196/47092. JMIR Pediatr Parent. 2024. PMID: 38329780 Free PMC article.
-
21st century (clinical) decision support in nursing and allied healthcare. Developing a learning health system: a reasoned design of a theoretical framework.BMC Med Inform Decis Mak. 2023 Dec 5;23(1):279. doi: 10.1186/s12911-023-02372-4. BMC Med Inform Decis Mak. 2023. PMID: 38053104 Free PMC article. Review.
-
Learning health systems.Semin Pediatr Surg. 2018 Dec;27(6):375-378. doi: 10.1053/j.sempedsurg.2018.10.005. Epub 2018 Oct 25. Semin Pediatr Surg. 2018. PMID: 30473042 Review.
Cited by
-
Building a learning health care community in rural and remote areas: a systematic review.BMC Health Serv Res. 2024 Sep 2;24(1):1013. doi: 10.1186/s12913-024-11194-7. BMC Health Serv Res. 2024. PMID: 39223608 Free PMC article.
-
Referral Decision Making of General Practitioners: A Signal Detection Study.Med Decis Making. 2019 Jan;39(1):21-31. doi: 10.1177/0272989X18813357. Med Decis Making. 2019. PMID: 30799690 Free PMC article.
-
A framework for analysing learning health systems: Are we removing the most impactful barriers?Learn Health Syst. 2019 Mar 21;3(4):e10189. doi: 10.1002/lrh2.10189. eCollection 2019 Oct. Learn Health Syst. 2019. PMID: 31641685 Free PMC article.
References
-
- Balogh EP, Miller BT, Ball JR, eds. Improving Diagnosis in Health Care. Washington, DC: The National Academies Press; 2015:450. - PubMed
-
- 2014 CBS report: malpractice risks in the diagnostic process: CRICO; 2015. Available from: https://www.rmf.harvard.edu/Clinician‐Resources/Article/2014/CBS‐Intro
-
- Carson‐Stevens A, Hibbert P, Williams H, et al. Characterising the nature of primary care patient safety incident reports in the England and Wales National Reporting and Learning System: a mixed‐methods agenda‐setting study for general practice. Health Serv Deliv Res. 2016;4(27):1‐76. - PubMed
LinkOut - more resources
Full Text Sources
