

The Impact on Ovarian Reserve of Different Hemostasis Methods in Laparoscopic Cystectomy: A Systematic Review and Meta-analysis
- PMID: 31247669
- PMCID: PMC10316829
- DOI: 10.1055/s-0039-1692697
The Impact on Ovarian Reserve of Different Hemostasis Methods in Laparoscopic Cystectomy: A Systematic Review and Meta-analysis
Abstract
Objective: The objective of this review was to analyze the impact on ovarian reserve of the different hemostatic methods used during laparoscopic cystectomy.
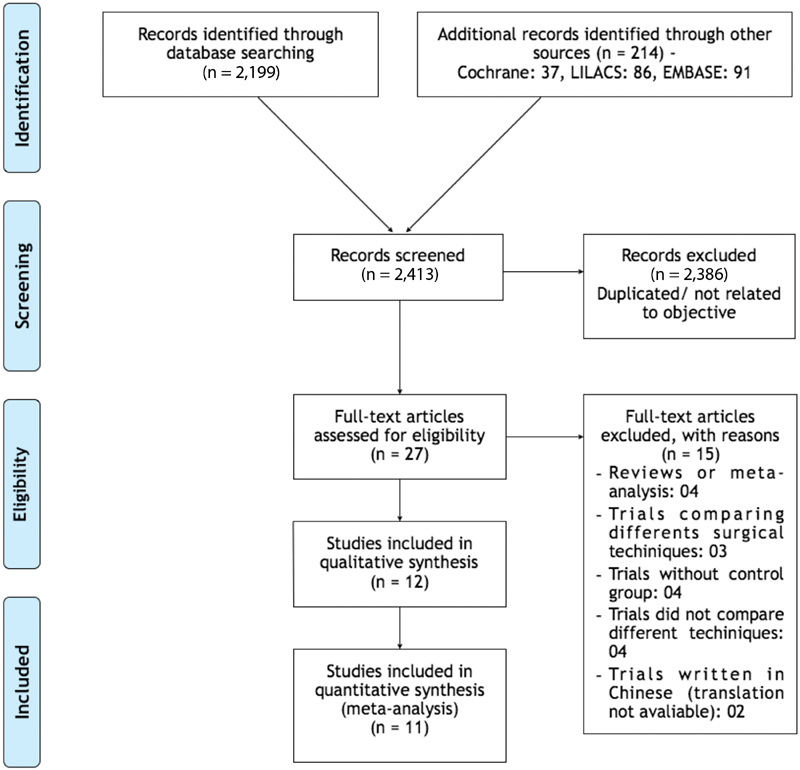
Data sources: The studies were identified by searching electronic databases (MEDLINE, Embase, Cochrane, LILACS) and scanning reference lists of articles.
Methods of study selection: We selected clinical trials that assessed the influence of hemostatic techniques on ovarian reserve in patients with ovarian cysts with benign sonographic appearance submitted to laparoscopic cystectomy by stripping technique. The included trials compared different laparoscopic hemostatic techniques: suture, bipolar electrocoagulation, ultrasonic energy and hemostatic sealants. The outcomes evaluated were level of serum anti-Mullerian hormone (AMH) and antral follicle count (AFC). The possibility of publication bias was evaluated by funnel plots.
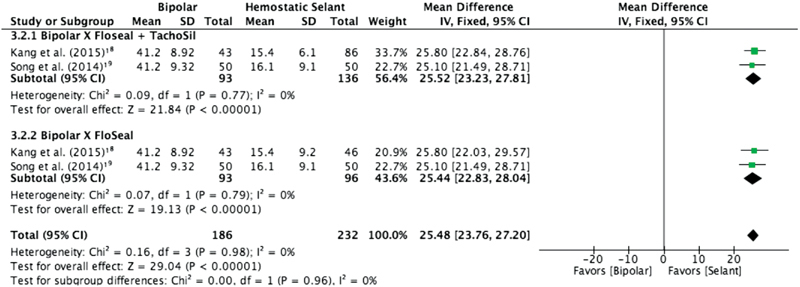
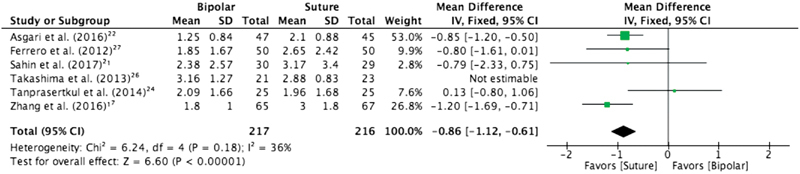
Tabulation, integration and results: Twelve trials involving 1,047 patients were evaluated. Laparoscopic suture was superior to bipolar coagulation when evaluating serum AMH and AFC, in the 1st, 3rd, 6th and 12th month after surgery. In the comparison between bipolar and hemostatic sealants, the results favored the use of hemostatic agents. The use of ultrasonic energy was not superior to the use of bipolar energy.
Conclusion: We recommend suture for hemostasis during laparoscopic cystectomy.
Objetivo: O objetivo desta revisão foi comparar o impacto dos diferentes métodos hemostáticos na reserva ovariana durante a ooforoplastia laparoscópica.
Fontes de dados: Os estudos foram identificados através da pesquisa de bases de dados eletrônicas (MEDLINE, Embase, Cochrane, LILACS) e listas de referência de artigos. SELEçãO DOS ESTUDOS: Selecionamos ensaios clínicos que avaliaram a influência das técnicas hemostáticas na reserva ovariana em pacientes com cistos ovarianos com aspecto ultrassonográfico benigno submetidos à ooforoplastia laparoscópica pela técnica de tração e contra-tração. Os estudos incluídos compararam as técnicas hemostáticas: sutura, energia bipolar, energia ultrassônica e selantes hemostáticos.
Coleta de dados: Os desfechos avaliados foram o hormônio antimülleriano e a contagem de folículos antrais. A possibilidade de viés de publicação foi avaliada por gráficos de funil. SíNTESE DOS DADOS: Doze estudos envolvendo 1.047 pacientes foram avaliados. A sutura foi superior à coagulação bipolar, e, na comparação entre selantes e energia bipolar, os resultados favoreceram o uso do primeiro grupo. O uso de energia ultrassônica não foi superior ao uso da energia bipolar. CONCLUSãO: Em conclusão, recomendamos a sutura para hemostasia durante a ooforoplastia laparoscópica.
Thieme Revinter Publicações Ltda Rio de Janeiro, Brazil.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures


Similar articles
-
Potential damage to ovarian reserve from laparoscopic electrocoagulation in endometriomas and benign ovarian cysts: a systematic review and meta-analysis.J Assist Reprod Genet. 2024 Oct;41(10):2727-2738. doi: 10.1007/s10815-024-03227-1. Epub 2024 Aug 15. J Assist Reprod Genet. 2024. PMID: 39145875
-
[Impact on ovarian reserve function by different homostasis methods during laparoscopic cystectomy in treatment of ovarian endometrioma].Zhonghua Fu Chan Ke Za Zhi. 2013 Jan;48(1):11-5. Zhonghua Fu Chan Ke Za Zhi. 2013. PMID: 23531244 Chinese.
-
Which Should Be the Preferred Technique During Laparoscopic Ovarian Cystectomy.Reprod Sci. 2017 Mar;24(3):393-399. doi: 10.1177/1933719116657195. Epub 2016 Jul 20. Reprod Sci. 2017. PMID: 27436368 Clinical Trial.
-
Effect on ovarian reserve of laparoscopic bipolar electrocoagulation versus laparotomic hemostatic sutures during unilateral ovarian cystectomy.Int J Gynaecol Obstet. 2011 Jul;114(1):69-72. doi: 10.1016/j.ijgo.2011.01.010. Epub 2011 Apr 6. Int J Gynaecol Obstet. 2011. PMID: 21474134 Clinical Trial.
-
Systematic Review and Meta-Analysis: Impact of Various Hemostasis Methods on Ovarian Reserve Function in Laparoscopic Cystectomy for Ovarian Endometriomas.Altern Ther Health Med. 2024 Aug;30(8):312-319. Altern Ther Health Med. 2024. PMID: 38064608
Cited by
-
Efficacy of ablation and sclerotherapy for the management of ovarian endometrioma: A narrative review.Clin Exp Reprod Med. 2022 Jun;49(2):76-86. doi: 10.5653/cerm.2021.05183. Epub 2022 May 4. Clin Exp Reprod Med. 2022. PMID: 35698769 Free PMC article.
-
Impact of Surgical Management of Endometrioma on AMH Levels and Pregnancy Rates: A Review of Recent Literature.J Clin Med. 2021 Jan 22;10(3):414. doi: 10.3390/jcm10030414. J Clin Med. 2021. PMID: 33499120 Free PMC article. Review.
-
Effects of intravenous tranexamic acid on ovarian reserve and intra-operative blood loss during laparoscopic cystectomy of endometriotic cyst: a pilot randomized controlled trial.Pilot Feasibility Stud. 2021 Sep 4;7(1):171. doi: 10.1186/s40814-021-00907-y. Pilot Feasibility Stud. 2021. PMID: 34481524 Free PMC article.
-
Preservation of the ovarian reserve and hemostasis during laparoscopic ovarian cystectomy by a hemostatic agent versus suturing for patients with ovarian endometriosis: study protocol for randomized controlled, non-inferiority trial (PRAHA-2 trial).Trials. 2021 Jul 21;22(1):473. doi: 10.1186/s13063-021-05431-1. Trials. 2021. PMID: 34289889 Free PMC article.
-
Ovarian Reserve After Robotic Versus Laparoscopic Single-Site Ovarian Cystectomy for Mature Cystic Teratoma: A Prospective Comparative Study.J Clin Med. 2025 May 29;14(11):3800. doi: 10.3390/jcm14113800. J Clin Med. 2025. PMID: 40507562 Free PMC article.
References
-
- Borgfeldt C, Andolf E.Transvaginal sonographic ovarian findings in a random sample of women 25-40 years old Ultrasound Obstet Gynecol 19991305345–350.. Doi: 10.1046/j.1469-0705.1999.13050345.x - PubMed
-
- Hart R J, Hickey M, Maouris P, Buckett W.Excisional surgery versus ablative surgery for ovarian endometriomata Cochrane Database Syst Rev 200802CD004992. Doi: 10.1002/14651858.CD004992.pub3 - PubMed
-
- Brun J L, Fritel X, Aubard Yet al.Management of presumed benign ovarian tumors: updated French guidelines Eur J Obstet Gynecol Reprod Biol 201418352–58.. Doi: 10.1016/j.ejogrb.2014.10.012 - PubMed
-
- Alborzi S, Foroughinia L, Kumar P V, Asadi N, Alborzi S.A comparison of histopathologic findings of ovarian tissue inadvertently excised with endometrioma and other kinds of benign ovarian cyst in patients undergoing laparoscopy versus laparotomy Fertil Steril 200992062004–2007.. Doi: 10.1016/j.fertnstert.2008.09.014 - PubMed
-
- Iwase A, Hirokawa W, Goto Met al.Serum anti-Müllerian hormone level is a useful marker for evaluating the impact of laparoscopic cystectomy on ovarian reserve Fertil Steril 201094072846–2849.. Doi: 10.1016/j.fertnstert.2010.06.010 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials