

Feasibility, Tolerability and Efficacy of Carfilzomib in Combination with Lenalidomide and Dexamethasone in Relapsed Refractory Myeloma Patients: A Retrospective Real-Life Survey of the Sicilian Myeloma Network
- PMID: 31248142
- PMCID: PMC6617295
- DOI: 10.3390/jcm8060877
Feasibility, Tolerability and Efficacy of Carfilzomib in Combination with Lenalidomide and Dexamethasone in Relapsed Refractory Myeloma Patients: A Retrospective Real-Life Survey of the Sicilian Myeloma Network
Abstract
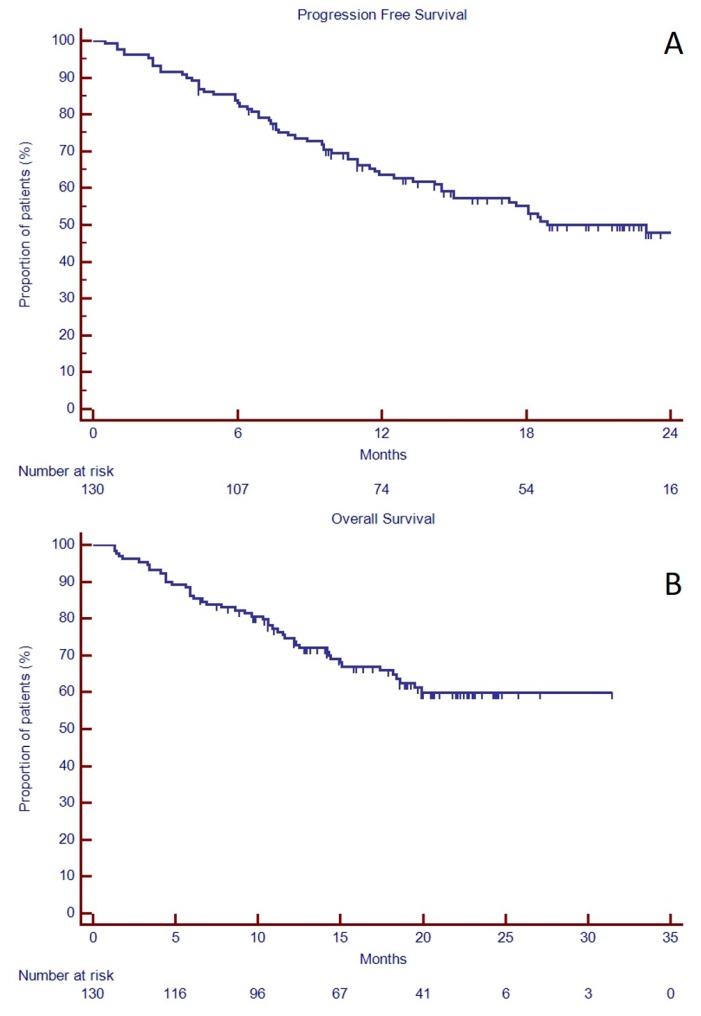
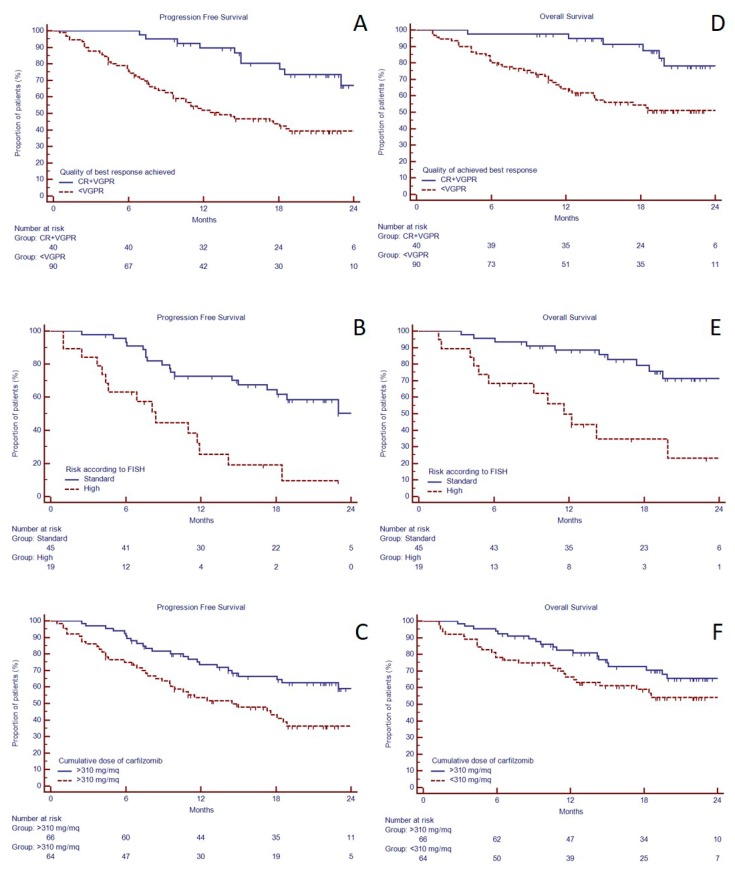
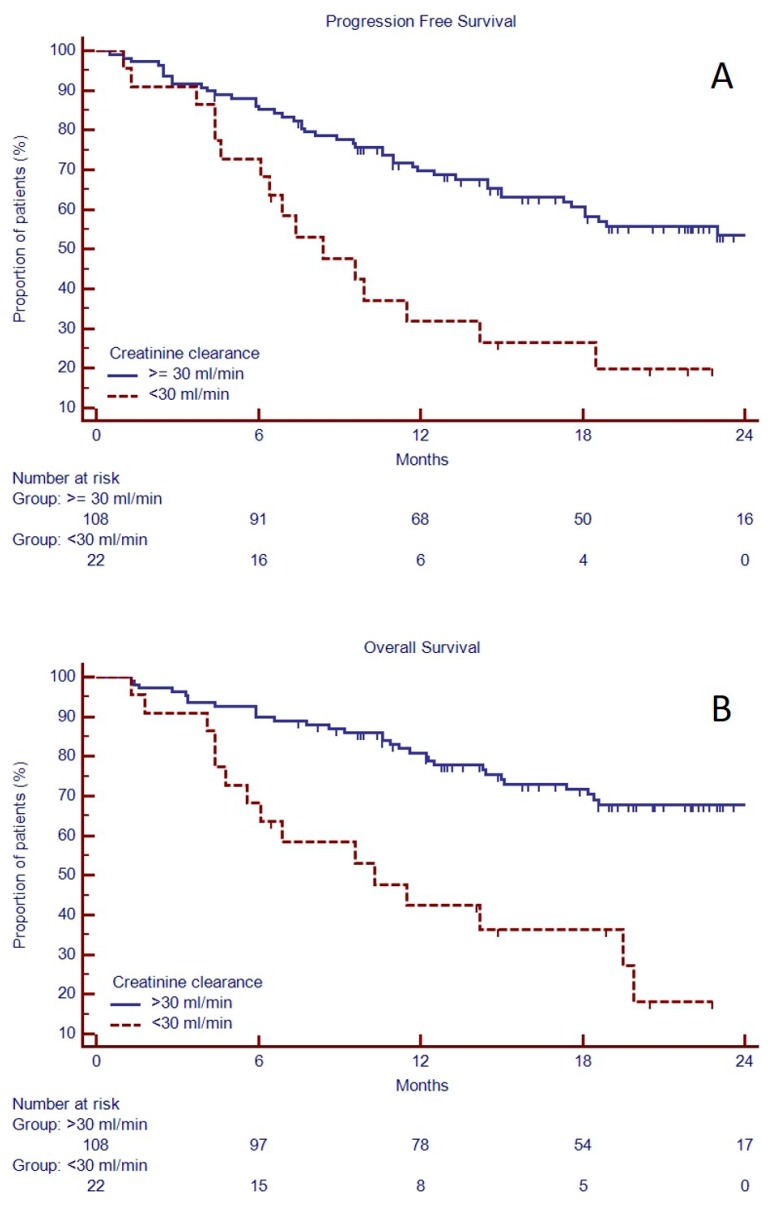
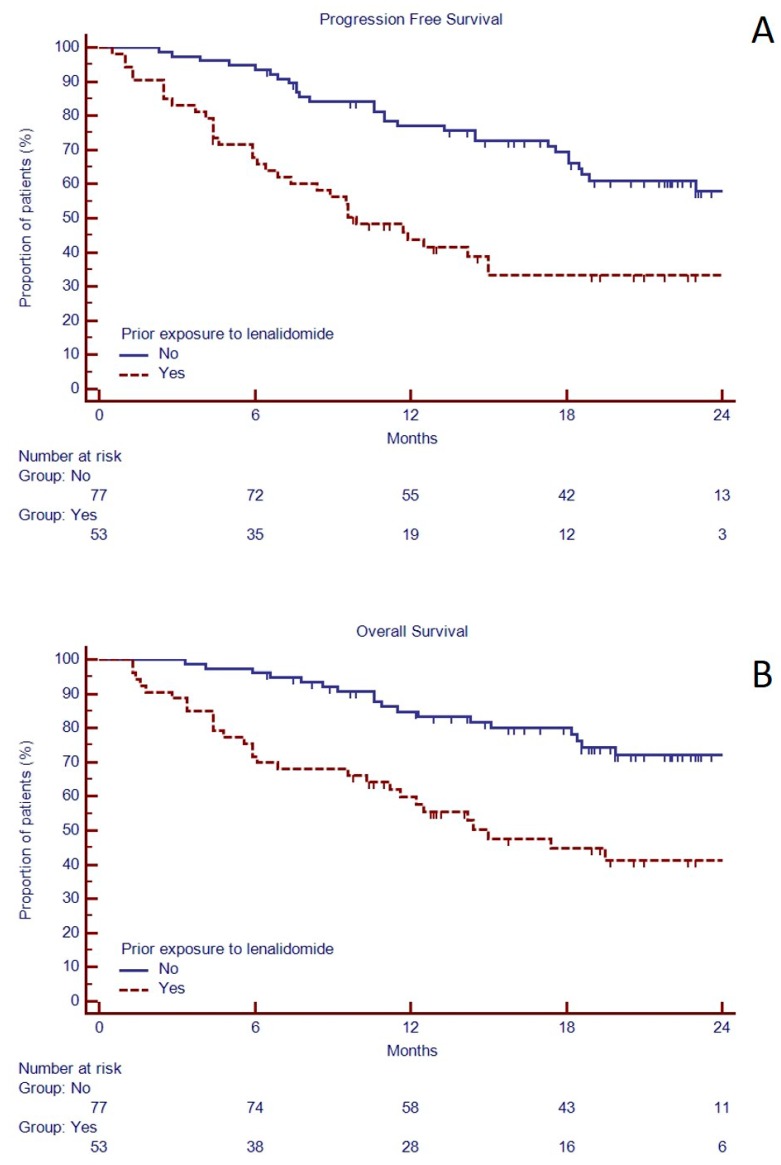
Background: The ASPIRE (NCT01080391) phase 3 trial showed the efficacy of carfilzomib, lenalidomide and dexamethasone (KRd) triplet for relapse and refractory multiple myeloma (RRMM). However, little is known about safety and efficacy of KRd outside a clinical trial context. Methods: Herein we report real life results of KRd given to 130 RRMM patients from 12 Sicilian Centers. Results: Median age was 62 years; patients had received a median of two previous lines of treatment (range 1-10) and 52% were refractory to previous treatment. Median number of KRd cycles was 12 (2-29), with a mean duration of treatment of 12 months; 21 patients had received at least 18 cycles. Overall response rate was 61%, including 18% complete response. Median PFS was 22.9 months, median OS was not reached. Creatinine clearance >30 mL/min, quality of the best achieved response and standard Fluorescence In Situ Hybridization (FISH) risk were independent predictors of favorable outcome. Patients who received the full-dosage of carfilzomib in the first two cycles had a better outcome. Conclusions: KRd was effective and well tolerated and in a considerable proportion of patients, therapy continued beyond the 18th cycle. The finding of a better outcome in patients with the higher cumulative dose of carfilzomib in the first two cycle encourages to maintain the maximum tolerated dose.
Keywords: KRd regimen; multiple myeloma; salvage therapy.
Conflict of interest statement
C.C., F.D.R., A.R., U.M. and V.L. received honoraria from Amgen. C.C., F.D.R. and A.R. received honoraria from Celgene. All the other authors declare no conflict of interest.
Figures
References
-
- Kumar S.K., Lee J.H., Lahuerta J.J., Morgan G., Richardson P.G., Crowley J., Haessler J., Feather J., Hoering A., Moreau P., et al. Risk of progression and survival in multiple myeloma relapsing after therapy with IMiDs and bortezomib: A multicenter international myeloma working group study. Leukemia. 2012;26:149–157. doi: 10.1038/leu.2011.196. - DOI - PMC - PubMed
-
- Dimopoulos M.A., Moreau P., Palumbo A., Joshua D., Pour L., Hájek R., Facon T., Ludwig H., Oriol A., Goldschmidt H., et al. Carfilzomib and dexamethasone versus bortezomib and dexamethasone for patients with relapsed or refractory multiple myeloma (ENDEAVOR): A randomised, phase 3, open-label, multicentre study. Lancet Oncol. 2016;17:27–38. doi: 10.1016/S1470-2045(15)00464-7. - DOI - PubMed
-
- San-Miguel J.F., Hungria V.T., Yoon S.S., Beksac M., Dimopoulos M.A., Elghandour A., Jedrzejczak W.W., Günther A., Nakorn T.N., Siritanaratkul N., et al. Panobinostat plus bortezomib and dexamethasone versus placebo plus bortezomib and dexamethasone in patients with relapsed or relapsed and refractory multiple myeloma: A multicentre, randomised, double-blind phase 3 trial. Lancet Oncol. 2014;15:1195–1206. doi: 10.1016/S1470-2045(14)70440-1. - DOI - PubMed
LinkOut - more resources
Full Text Sources
