

Elevated Mitral Valve Pressure Gradient Is Predictive of Long-Term Outcome After Percutaneous Edge-to-Edge Mitral Valve Repair in Patients With Degenerative Mitral Regurgitation ( MR ), But Not in Functional MR
- PMID: 31248323
- PMCID: PMC6662353
- DOI: 10.1161/JAHA.118.011366
Elevated Mitral Valve Pressure Gradient Is Predictive of Long-Term Outcome After Percutaneous Edge-to-Edge Mitral Valve Repair in Patients With Degenerative Mitral Regurgitation ( MR ), But Not in Functional MR
Abstract
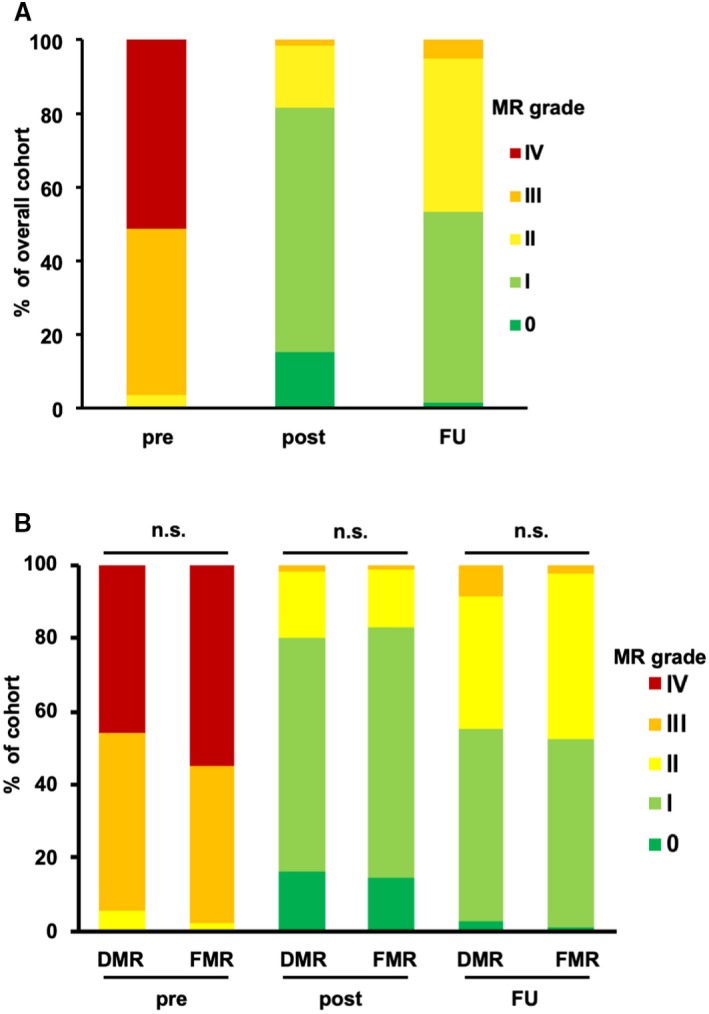
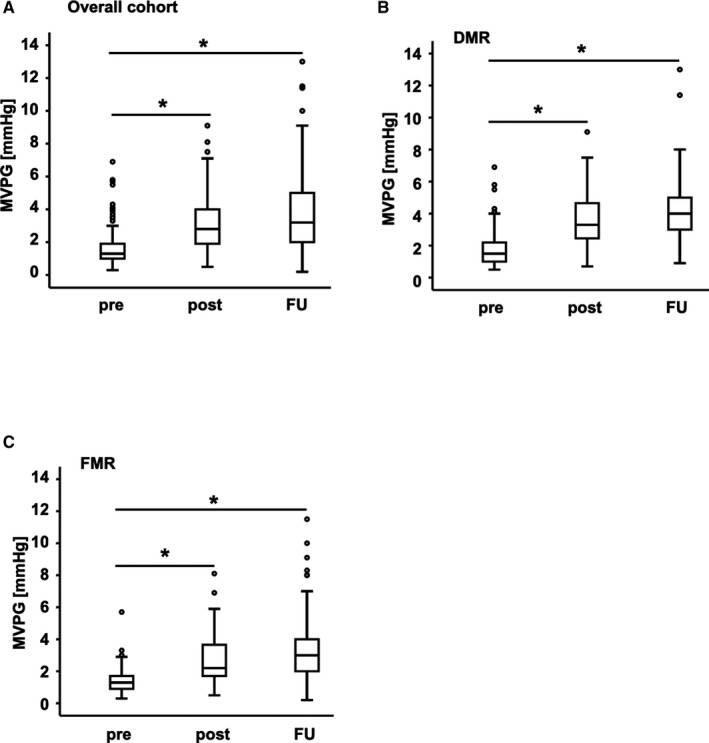
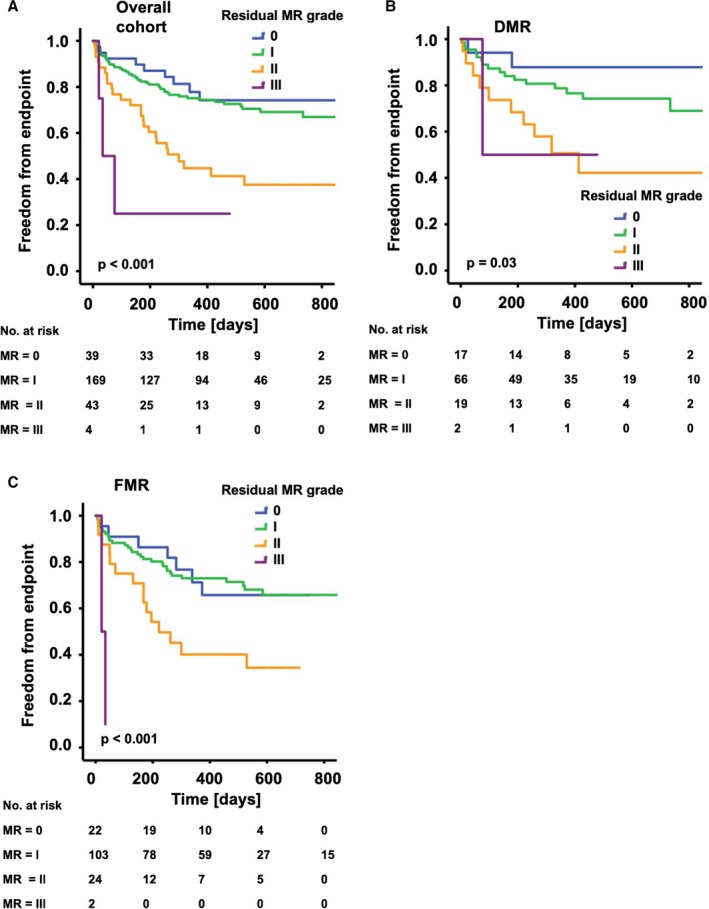
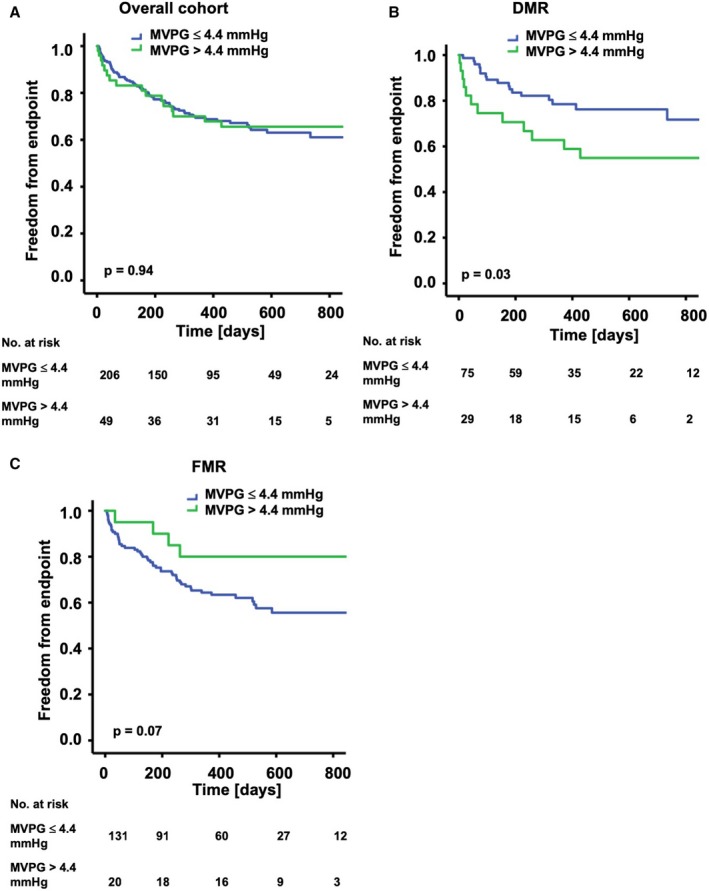
Background This study analyzed the effects on long-term outcome of residual mitral regurgitation ( MR ) and mean mitral valve pressure gradient ( MVPG ) after percutaneous edge-to-edge mitral valve repair using the MitraClip system. Methods and Results Two hundred fifty-five patients who underwent percutaneous edge-to-edge mitral valve repair were analyzed. Kaplan-Meier and Cox regression analyses were performed to evaluate the impact of residual MR and MVPG on clinical outcome. A combined clinical end point (all-cause mortality, MV surgery, redo procedure, implantation of a left ventricular assist device) was used. After percutaneous edge-to-edge mitral valve repair, mean MVPG increased from 1.6±1.0 to 3.1±1.5 mm Hg ( P<0.001). Reduction of MR severity to ≤2+ postintervention was achieved in 98.4% of all patients. In the overall patient cohort, residual MR was predictive of the combined end point while elevated MVPG >4.4 mm Hg was not according to Kaplan-Meier and Cox regression analyses. We then analyzed the cohort with degenerative and that with functional MR separately to account for these different entities. In the cohort with degenerative MR , elevated MVPG was associated with increased occurrence of the primary end point, whereas this was not observed in the cohort with functional MR . Conclusions MVPG >4.4 mm Hg after MitraClip implantation was predictive of clinical outcome in the patient cohort with degenerative MR . In the patient cohort with functional MR , MVPG >4.4 mm Hg was not associated with increased clinical events.
Keywords: mitral stenosis; mitral valve; mitral valve regurgitation; percutaneous mitral valve repair; percutaneous treatment.
Figures
References
-
- Feldman T, Kar S, Elmariah S, Smart SC, Trento A, Siegel RJ, Apruzzese P, Fail P, Rinaldi MJ, Smalling RW, Hermiller JB, Heimansohn D, Gray WA, Grayburn PA, Mack MJ, Lim DS, Ailawadi G, Herrmann HC, Acker MA, Silvestry FE, Foster E, Wang A, Glower DD, Mauri L; EVEREST II Investigators . Randomized comparison of percutaneous repair and surgery for mitral regurgitation: 5‐year results of EVEREST II. J Am Coll Cardiol. 2015;66:2844–2854. - PubMed
-
- Nickenig G, Estevez‐Loureiro R, Franzen O, Tamburino C, Vanderheyden M, Luscher TF, Moat N, Price S, Dall'Ara G, Winter R, Corti R, Grasso C, Snow TM, Jeger R, Blankenberg S, Settergren M, Tiroch K, Balzer J, Petronio AS, Buttner HJ, Ettori F, Sievert H, Fiorino MG, Claeys M, Ussia GP, Baumgartner H, Scandura S, Alamgir F, Keshavarzi F, Colombo A, Maisano F, Ebelt H, Aruta P, Lubos E, Plicht B, Schueler R, Pighi M, Di Mario C; Transcatheter Valve Treatment Sentinel Registry Investigators of the EURObservational Research Programme of the European Society of Cardiology . Percutaneous mitral valve edge‐to‐edge repair: in‐hospital results and 1‐year follow‐up of 628 patients of the 2011–2012 Pilot European Sentinel Registry. J Am Coll Cardiol. 2014;64:875–884. - PubMed
-
- Nishimura RA, Vahanian A, Eleid MF, Mack MJ. Mitral valve disease—current management and future challenges. Lancet. 2016;387:1324–1334. - PubMed
-
- Rudolph V, Huntgeburth M, von Bardeleben RS, Boekstegers P, Lubos E, Schillinger W, Ouarrak T, Eggebrecht H, Butter C, Plicht B, May A, Franzen O, Schofer J, Senges J, Baldus S. Clinical outcome of critically ill, not fully recompensated, patients undergoing MitraClip therapy. Eur J Heart Fail. 2014;16:1223–1229. - PubMed
-
- Stone GW, Lindenfeld J, Abraham WT, Kar S, Lim DS, Mishell JM, Whisenant B, Grayburn PA, Rinaldi M, Kapadia SR, Rajagopal V, Sarembock IJ, Brieke A, Marx SO, Cohen DJ, Weissman NJ, Mack MJ; Investigators C . Transcatheter mitral‐valve repair in patients with heart failure. N Engl J Med. 2018;379:2307–2318. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
