

Hypothermic Oxygenated Machine Perfusion of Liver Grafts from Brain-Dead Donors
- PMID: 31249370
- PMCID: PMC6597580
- DOI: 10.1038/s41598-019-45843-3
Hypothermic Oxygenated Machine Perfusion of Liver Grafts from Brain-Dead Donors
Abstract
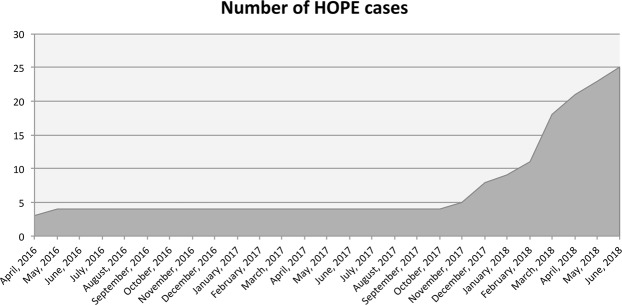
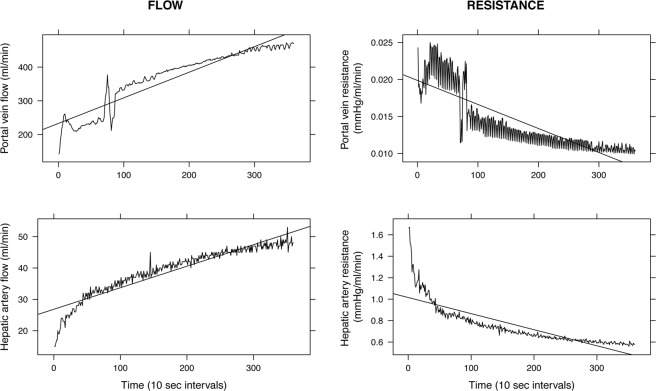
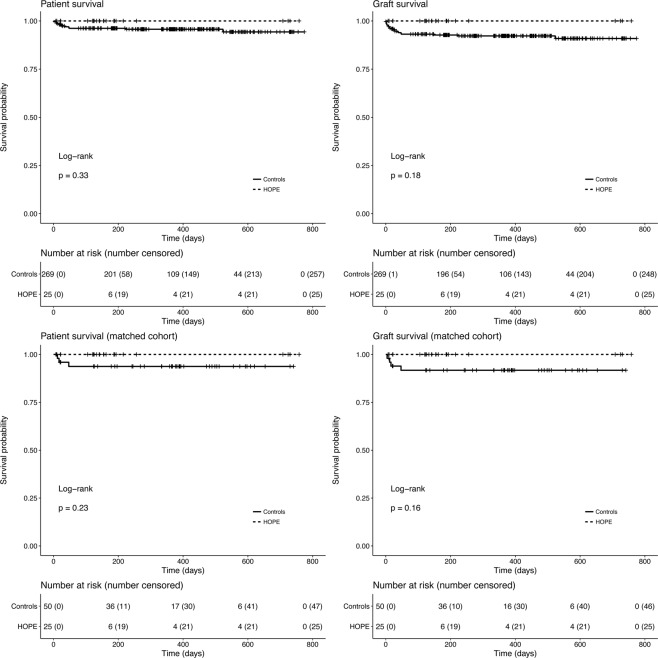
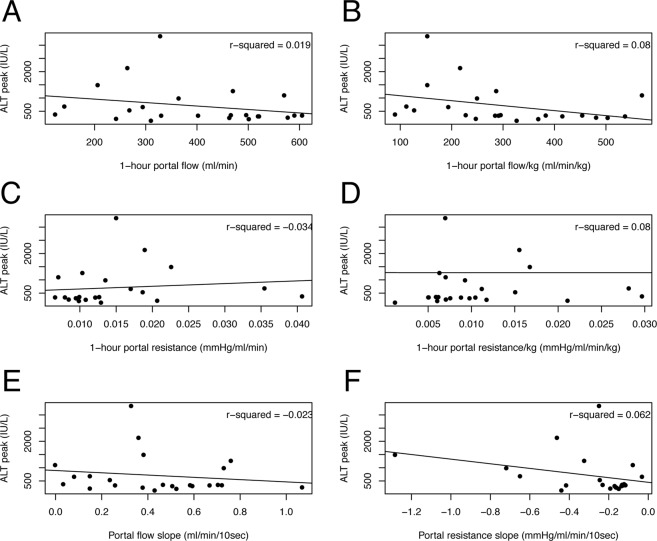
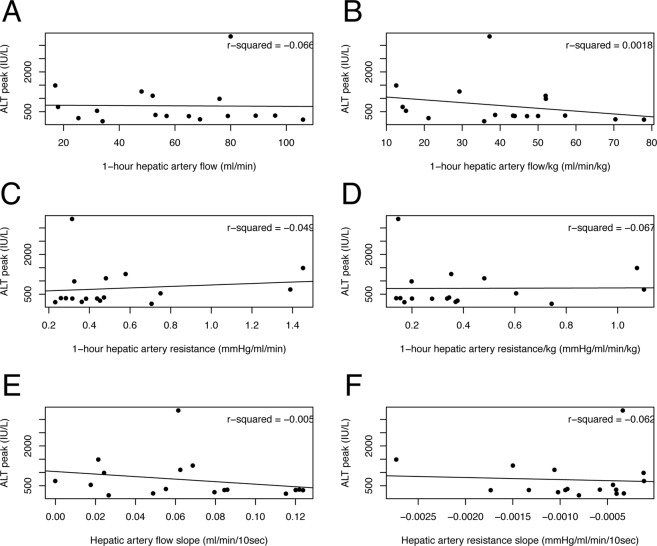
Hypothermic oxygenated machine perfusion (HOPE) was introduced in liver transplantation (LT) to mitigate ischemia-reperfusion injury. Available clinical data mainly concern LT with donors after circulatory-determined death, whereas data on brain-dead donors (DBD) are scarce. To assess the impact of end-ischemic HOPE in DBD LT, data on primary adult LTs performed between March 2016 and June 2018 were analyzed. HOPE was used in selected cases of donor age >80 years, apparent severe graft steatosis, or ischemia time ≥10 hours. Outcomes of HOPE-treated cases were compared with those after static cold storage. Propensity score matching (1:2) and Bayesian model averaging were used to overcome selection bias. During the study period, 25 (8.5%) out of 294 grafts were treated with HOPE. After matching, HOPE was associated with a lower severe post-reperfusion syndrome (PRS) rate (4% versus 20%, p = 0.13) and stage 2-3 acute kidney injury (AKI) (16% versus 42%, p = 0.046). Furthermore, Bayesian model averaging showed lower transaminases peak and a lower early allograft dysfunction (EAD) rate after HOPE. A steeper decline in arterial graft resistance throughout perfusion was associated with lower EAD rate. HOPE determines a significant reduction of ischemia reperfusion injury in DBD LT.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Cameron Andrew M., Ghobrial R Mark, Yersiz Hasan, Farmer Douglas G., Lipshutz Gerald S., Gordon Sherilyn A., Zimmerman Michael, Hong Johnny, Collins Thomas E., Gornbein Jeffery, Amersi Farin, Weaver Michael, Cao Carlos, Chen Tony, Hiatt Jonathan R., Busuttil Ronald W. Optimal Utilization of Donor Grafts With Extended Criteria. Annals of Surgery. 2006;243(6):748–755. doi: 10.1097/01.sla.0000219669.84192.b3. - DOI - PMC - PubMed
-
- Ghinolfi Davide, Tincani Giovanni, Rreka Erion, Roffi Niccolo’, Coletti Laura, Balzano Emanuele, Catalano Gabriele, Meli Sonia, Carrai Paola, Petruccelli Stefania, Biancofiore Gianni, Filipponi Franco, De Simone Paolo. Dual aortic and portal perfusion at procurement prevents ischaemic-type biliary lesions in liver transplantation when using octogenarian donors: a retrospective cohort study. Transplant International. 2018;32(2):193–205. doi: 10.1111/tri.13342. - DOI - PubMed
