

Hypoxia Imaging and Adaptive Radiotherapy: A State-of-the-Art Approach in the Management of Glioma
- PMID: 31249831
- PMCID: PMC6582242
- DOI: 10.3389/fmed.2019.00117
Hypoxia Imaging and Adaptive Radiotherapy: A State-of-the-Art Approach in the Management of Glioma
Abstract
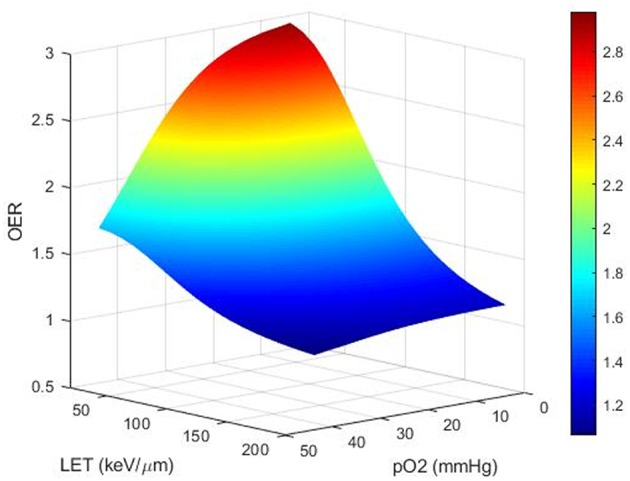
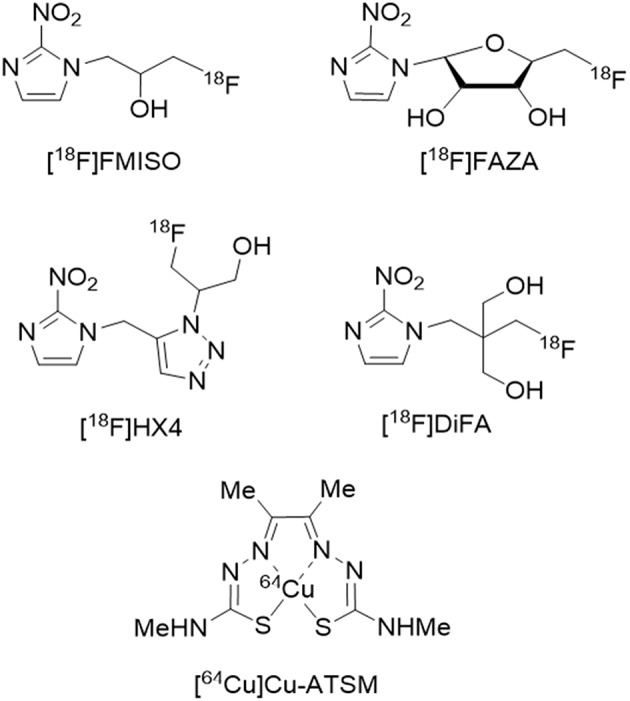
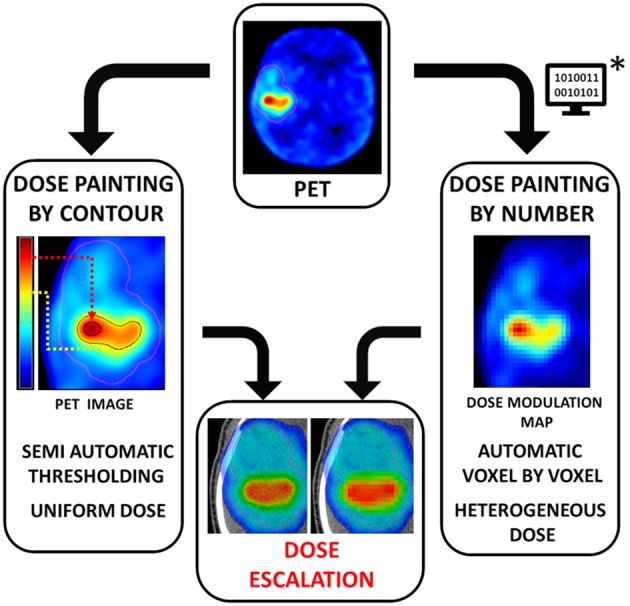
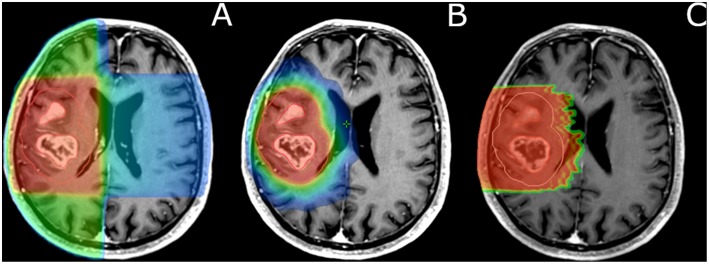
Severe hypoxia [oxygen partial pressure (pO2) below 5-10 mmHg] is more frequent in glioblastoma multiforme (GBM) compared to lower-grade gliomas. Seminal studies in the 1950s demonstrated that hypoxia was associated with increased resistance to low-linear energy transfer (LET) ionizing radiation. In experimental conditions, the total radiation dose has to be multiplied by a factor of 3 to achieve the same cell lethality in anoxic situations. The presence of hypoxia in human tumors is assumed to contribute to treatment failures after radiotherapy (RT) in cancer patients. Therefore, a logical way to overcome hypoxia-induced radioresistance would be to deliver substantially higher doses of RT in hypoxic volumes delineated on pre-treatment imaging as biological target volumes (BTVs). Such an approach faces various fundamental, technical, and clinical challenges. The present review addresses several technical points related to the delineation of hypoxic zones, which include: spatial accuracy, quantitative vs. relative threshold, variations of hypoxia levels during RT, and availability of hypoxia tracers. The feasibility of hypoxia imaging as an assessment tool for early tumor response to RT and for predicting long-term outcomes is discussed. Hypoxia imaging for RT dose painting is likewise examined. As for the radiation oncologist's point of view, hypoxia maps should be converted into dose-distribution objectives for RT planning. Taking into account the physics and the radiobiology of various irradiation beams, preliminary in silico studies are required to investigate the feasibility of dose escalation in terms of normal tissue tolerance before clinical trials are undertaken.
Keywords: MRI; PET; glioblastoma; hypoxia; imaging; radiation therapy.
Figures
References
-
- Simpson-Herren L, Lloyd HH. Kinetic parameters and growth curves for experimental tumor systems. Cancer Chemother. Rep. (1970) 54:143–74. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials