

Orodispersible minitablets of enalapril for use in children with heart failure (LENA): Rationale and protocol for a multicentre pharmacokinetic bridging study and follow-up safety study
- PMID: 31249901
- PMCID: PMC6586986
- DOI: 10.1016/j.conctc.2019.100393
Orodispersible minitablets of enalapril for use in children with heart failure (LENA): Rationale and protocol for a multicentre pharmacokinetic bridging study and follow-up safety study
Abstract
Introduction: Treatment of paediatric heart failure is based on paradigms extensively tested in the adult population assuming similar underlying pathophysiological mechanisms. Angiotensin converting enzyme inhibitors (ACEI) like enalapril are one of the cornerstones of treatment and commonly used off-label in children. Dose recommendations have been extrapolated from adult experience, but the relationship between dose and pharmacokinetics (PK) in (young) children is insufficiently studied. Furthermore, appropriate paediatric formulations are lacking. Within the European collaborative project LENA, a novel formulation of enalapril orodispersible minitablets (ODMT), suitable for paediatric administration, will be tested in (young) children with heart failure due to either dilated cardiomyopathy or congenital heart disease in two pharmacokinetic bridging studies. Paediatric PK data of enalapril and its active metabolite enalaprilat will be obtained. In a follow-up study, the safety of enalapril ODMTs will be demonstrated in patients on long-term treatment of up to 10 months. Furthermore, additional information about pharmacodynamics (PD) and ODMT acceptability will be collected in all three studies.
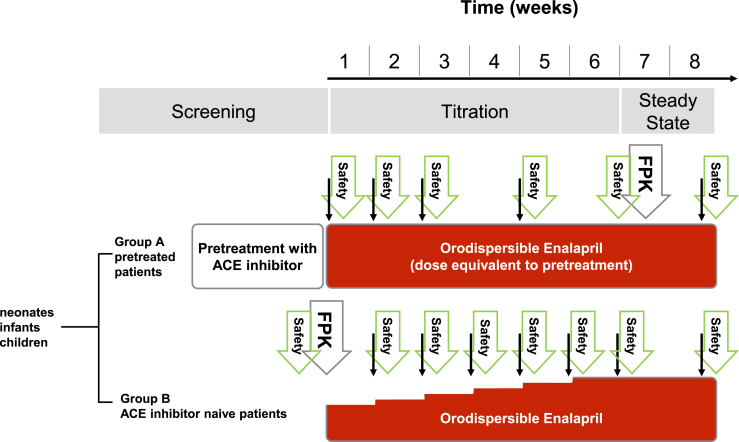
Methods and analysis: Phase II/III, open-label, multicentre study. Children with dilated cardiomyopathy (DCM) (n = 25; 1 month to less than 12 years) or congenital heart disease (CHD) (n = 60; 0 to less than 6 years) requiring or already on ACEI will be included. Exclusion criteria include severe heart failure precluding ACEI use, hypotension, renal impairment, hypersensitivity to ACEI. For those naïve to ACEI up-titration to an optimal dose will be performed, those already on ACEI will be switched to an expected equivalent dose of enalapril ODMT and optimised. In the first 8 weeks of treatment, a PK profile will be obtained at the first dose (ACEI naïve patients) or when an optimal dose is reached. Furthermore, population PK will be done with concentrations detected over the whole treatment period. PD and safety data will be obtained at least at 2-weeks intervals. Subsequently, an intended number of 85 patients will be followed-up up to 10 months to demonstrate long-term safety, based on the occurrence of (severe) adverse events and monitoring of vital signs and renal function.
Ethics and dissemination: Clinical Trial Authorisation and a favourable ethics committee opinion were obtained in all five participating countries. Results of the studies will be submitted for publication in a peer-reviewed journal.
Trial registration numbers: EudraCT 2015-002335-17, EudraCT 2015-002396-18, EudraCT 2015-002397-21.
Keywords: Clinical pharmacology; Congenital heart disease; Dilated cardiomyopathy; Heart failure; Paediatric cardiology.
Figures
References
-
- Ross R.D., Daniels S.R., Schwartz D.C. Plasma norepinephrine levels in infants and children with congestive heart failure. Am. J. Cardiol. 1987;59(8):911–914. - PubMed
-
- Auslender M., Artman M. Overview of the management of pediatric heart failure. Prog. Pediatr. Cardiol. 2000;11(3):231–241. - PubMed
-
- Kirk R., Dipchand A.I., Rosenthal D.N. The International Society of Heart and Lung Transplantation Guidelines for the management of pediatric heart failure: executive summary. J. Heart Lung Transplant. 2014;33:888–909. - PubMed
-
- Sommers C., Nagel B.H., Neudorf U. Congestive Heart Failure in Childhood. An Epidemiologic Study; Herzinsuffizienz im Kindesalter. Eine epidemiologische Studie. Herz. 2005 Oct 1;30(7):652. - PubMed
LinkOut - more resources
Full Text Sources
