

Reversible cutaneous silent period abnormalities in vitamin B12 deficiency: A case report
- PMID: 31249907
- PMCID: PMC6586985
- DOI: 10.1016/j.cnp.2019.05.002
Reversible cutaneous silent period abnormalities in vitamin B12 deficiency: A case report
Abstract
Objectives: Vitamin B12 deficiency is common in adult and elderly patients and is often underdiagnosed because of its polymorphous manifestations. Neurological symptoms of this condition include subacute combined degeneration and polyneuropathy, with possible affection of thin-myelinated A-delta fibers. Cutaneous silent periods (CSPs) may serve to test small-diameter fiber function non-invasively, using routine electrodiagnostic equipment, but to the best of our knowledge have not been studied so far in vitamin B12 deficiency.
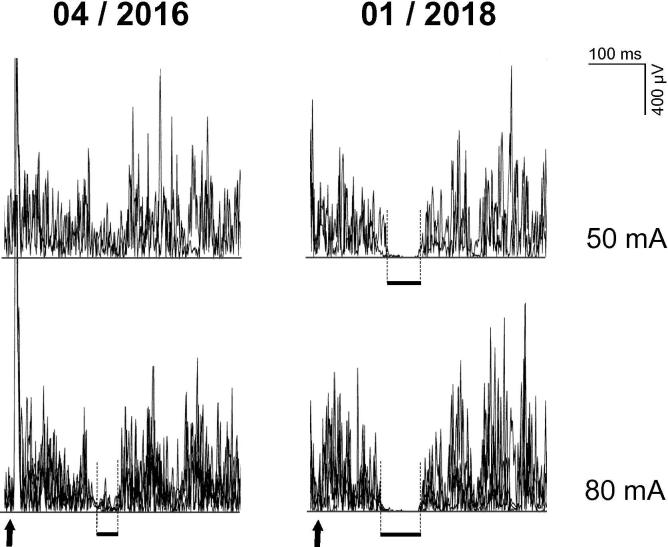
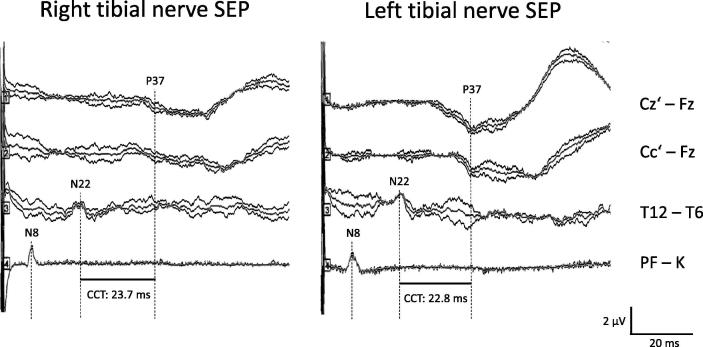
Methods: We report a 49-year-old male patient suffering from B12 hypovitaminosis due to autoantibodies against gastric parietal cells, who underwent neurophysiological investigation to confirm clinically suspected polyneuropathy during the first month of intramuscular vitamin B12 supplementation. We performed standard electroneurography, needle electromyography in tibialis anterior muscle, quantitative sensory testing, and cutaneous silent periods six months after symptom onset and repeated the electrodiagnostic study 21 months later, after intramuscular vitamin B12 supplementation.
Results: Standard electroneurography demonstrated axonal sensory polyneuropathy. Needle electromyography (EMG) in tibialis anterior muscle was unremarkable. Cutaneous silent periods in tibialis anterior muscle after noxious electrical sural nerve stimulation were delayed, with incomplete EMG suppression concurring with dysfunction of thin-myelinated A-delta fibers. Quantitative sensory testing revealed altered cold and warm perception thresholds in both upper limbs, but normal values in both lower limbs. A follow-up electrodiagnostic study after 21 months intramuscular vitamin B12 supplementation revealed improvement of all neurophysiological findings, including normalization of cutaneous silent periods.
Conclusions: Thin-myelinated A-delta fibers may be affected in B12 hypovitaminosis and may show recovery after intramuscular vitamin B12 supplementation. CSP may serve to diagnose small fiber affection in this medical condition and to monitor their recovery after vitamin supplementation.
Significance: CSP testing represents a useful, non-invasive, rapidly available diagnostic and follow-up tool in vitamin B12 deficiency.
Keywords: A-delta fiber; Cutaneous silent period; Nerve conduction; Polyneuropathy; Quantitative sensory testing; Vitamin B12 deficiency.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Allen L.H. How common is vitamin B-12 deficiency? Am. J. Clin. Nutr. 2009;89(2):693S–696S. - PubMed
-
- Carmel R. Pernicious anemia. In: Johnson L.R., editor. Encyclopedia of Gastroenterology. Academic Press; Waltham, MA: 2004. pp. 170–171.
-
- Chan A.C., Wilder-Smith E.P. Small fiber neuropathy: getting bigger! Muscle Nerve. 2016;53(5):671–682. - PubMed
-
- Fine E.J., Soria E.D. Myths about vitamin B12 deficiency. South. Med. J. 1991;84(12):1475–1481. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
