

Sensitivity of a Simple Noninvasive Screening Algorithm for Chronic Thromboembolic Pulmonary Hypertension after Acute Pulmonary Embolism
- PMID: 31249932
- PMCID: PMC6524865
- DOI: 10.1055/s-0038-1636537
Sensitivity of a Simple Noninvasive Screening Algorithm for Chronic Thromboembolic Pulmonary Hypertension after Acute Pulmonary Embolism
Abstract
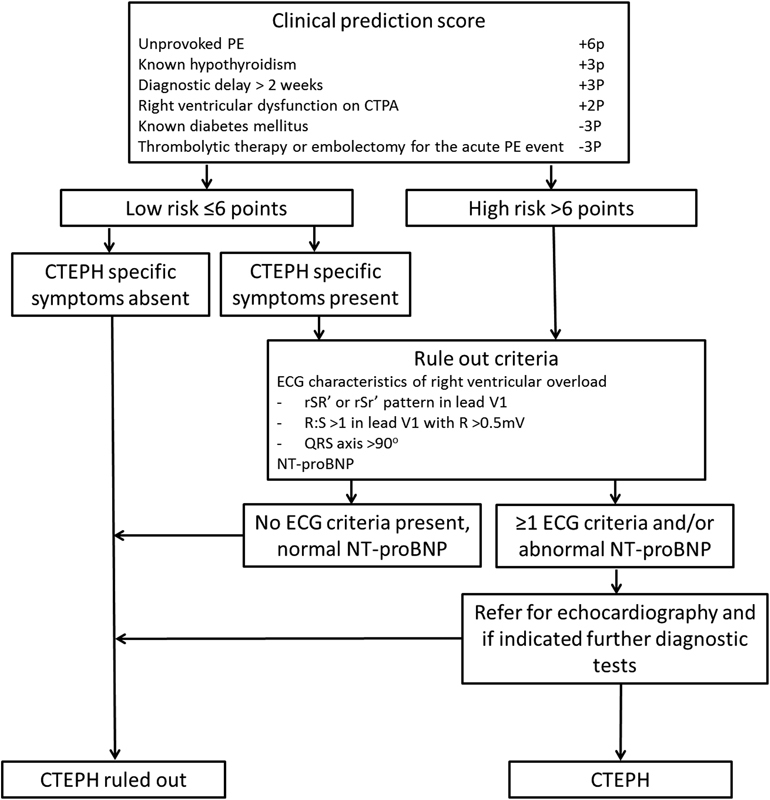
Background Recently, we constructed a noninvasive screening algorithm aiming at earlier chronic thromboembolic pulmonary hypertension (CTEPH) detection after acute pulmonary embolism (PE), consisting of a prediction score and combined electrocardiography (ECG)/N-terminal pro-brain natriuretic peptide (NT-proBNP) assessment. The aim of this study was to confirm the algorithm's sensitivity for CTEPH detection and to evaluate the reproducibility of its individual items. Methods Two independent researchers calculated the prediction score in 54 consecutive patients with a history of acute PE and proven CTEPH based on clinical characteristics at PE diagnosis, and evaluated the ECG and NT-proBNP level assessed at the moment of CTEPH diagnosis. Interobserver agreement for the assessment of the prediction score, right-to-left ventricle (RV/LV) ratio measurement on computed tomography pulmonary angiography, as well as ECG reading was evaluated by calculating Cohen's kappa statistics. Results Median time between PE diagnosis and presentation with CTEPH was 9 months (interquartile range: 5-15). The sensitivity of the algorithm was found to be 91% (95% confidence interval [CI]: 79-97%), indicating that 27 of 30 cases of CTEPH would have been detected when applying the screening algorithm to 1,000 random PE survivors with a 3% CTEPH incidence (projected negative predictive value: 99.7%; 95% CI: 99.1-99.9%). The interobserver agreement for calculating the prediction score, RV/LV ratio measurement, and ECG reading was excellent with a kappa of 0.96, 0.95, and 0.89, respectively. Conclusion The algorithm had a high sensitivity of 91% and was highly reproducible. Prospective validation of the algorithm in consecutive PE patients is required before it can be used in clinical practice.
Keywords: CTEPH; pulmonary embolism; reproducibility; screening algorithm; sensitivity.
Conflict of interest statement
Figures

References
-
- Galiè N, Humbert M, Vachiery J L et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Respir J. 2015;46(04):903–975. - PubMed
-
- Mayer E, Jenkins D, Lindner J et al. Surgical management and outcome of patients with chronic thromboembolic pulmonary hypertension: results from an international prospective registry. J Thorac Cardiovasc Surg. 2011;141(03):702–710. - PubMed
-
- Delcroix M, Lang I, Pepke-Zaba J et al. Long-term outcome of patients with chronic thromboembolic pulmonary hypertension: results from an international prospective registry. Circulation. 2016;133(09):859–871. - PubMed
-
- Tscholl D, Langer F, Wendler O, Wilkens H, Georg T, Schäfers H J. Pulmonary thromboendarterectomy--risk factors for early survival and hemodynamic improvement. Eur J Cardiothorac Surg. 2001;19(06):771–776. - PubMed
-
- Kunihara T, Gerdts J, Groesdonk H et al. Predictors of postoperative outcome after pulmonary endarterectomy from a 14-year experience with 279 patients. Eur J Cardiothorac Surg. 2011;40(01):154–161. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
