

Direct Oral Anticoagulants or Standard Anticoagulant Therapy in Fragile Patients with Venous Thromboembolism
- PMID: 31249985
- PMCID: PMC6524917
- DOI: 10.1055/s-0039-1683970
Direct Oral Anticoagulants or Standard Anticoagulant Therapy in Fragile Patients with Venous Thromboembolism
Abstract
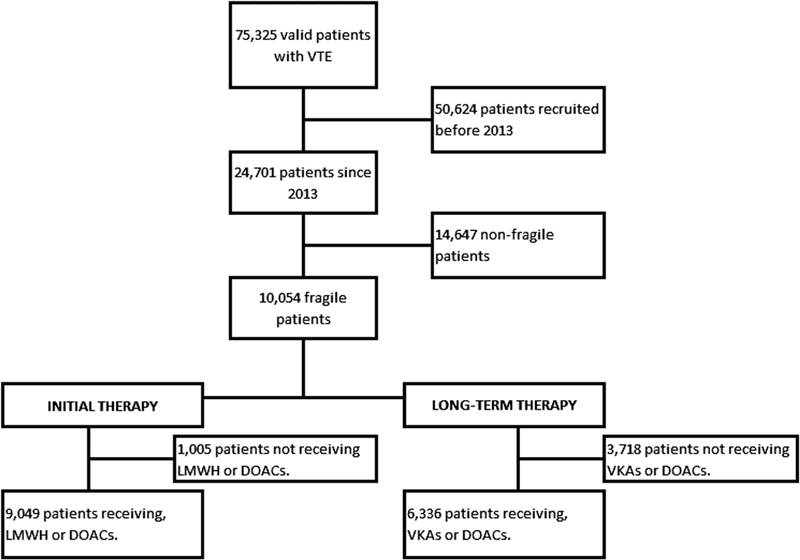
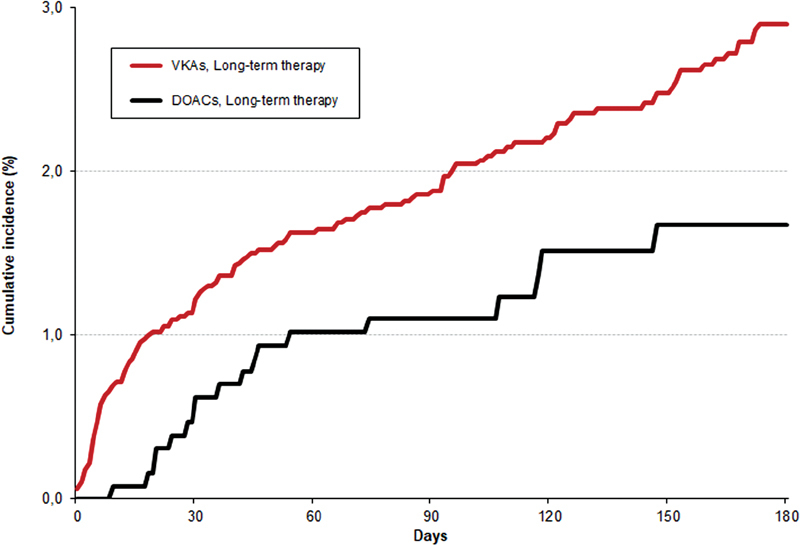
Background The efficacy and safety of the direct oral anticoagulants (DOACs) in fragile patients (age ≥ 75 years and/or creatinine clearance levels ≤ 50 mL/min and/or body weight ≤ 50kg) with venous thromboembolism (VTE) has not been evaluated. Methods We used the RIETE database to compare the rates of the composite of VTE recurrences or major bleeding during anticoagulation in fragile patients with VTE, according to the use of DOACs or standard anticoagulant therapy. Results From January 2013 to April 2018, 24,701 patients were recruited. Of these, 10,054 (41%) were fragile. Initially, 473 fragile patients (4.7%) received DOACs and 8,577 (85%) low-molecular-weight heparin (LMWH). For long-term therapy, 1,298 patients (13%) received DOACs and 5,038 (50%) vitamin K antagonists (VKAs). Overall, 95 patients developed VTE recurrences and 262 had major bleeding. Patients initially receiving DOACs had a lower rate of the composite outcome (hazard ratio [HR]: 0.32; 95% confidence interval [CI]: 0.08-0.88) than those on LMWH. Patients receiving DOACs for long-term therapy had a nonsignificantly lower rate of the composite outcome (HR: 0.70; 95% CI: 0.46-1.03) than those on VKAs. On multivariable analysis, patients initially receiving DOACs had a nonsignificantly lower risk for the composite outcome (HR: 0.36; 95% CI: 0.11-1.15) than those on LMWH, while those receiving DOACs for long-term therapy had a significantly lower risk (HR: 0.61; 95% CI: 0.41-0.92) than those on VKAs. Conclusions Our data suggest that the use of DOACs may be more effective and safe than standard therapy in fragile patients with VTE, a subgroup of patients where the risk for bleeding is particularly high.
Keywords: direct oral anticoagulants; fragile patients; venous thromboembolism.
Conflict of interest statement
Figures
References
-
- Bauersachs R, Berkowitz S D, Brenner B et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med. 2010;363(26):2499–2510. - PubMed
-
- Büller H R, Décousus H, Grosso M A et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med. 2013;369(15):1406–1415. - PubMed
-
- Ruíz-Giménez N, Suárez C, González R et al. Predictive variables for major bleeding events in patients presenting with documented acute venous thromboembolism. Findings from the RIETE Registry. Thromb Haemost. 2008;100(01):26–31. - PubMed
-
- Muñoz-Torrero J F, Bounameaux H, Pedrajas J Met al. Effects of age on the risk of dying from pulmonary embolism or bleeding during treatment of deep vein thrombosis J Vasc Surg 20115406, Suppl):26S–32S. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
