

Trends in Health Equity in the United States by Race/Ethnicity, Sex, and Income, 1993-2017
- PMID: 31251377
- PMCID: PMC6604079
- DOI: 10.1001/jamanetworkopen.2019.6386
Trends in Health Equity in the United States by Race/Ethnicity, Sex, and Income, 1993-2017
Erratum in
-
Incorrect Wording in Results.JAMA Netw Open. 2019 Jul 3;2(7):e199357. doi: 10.1001/jamanetworkopen.2019.9357. JAMA Netw Open. 2019. PMID: 31339536 Free PMC article. No abstract available.
Abstract
Importance: Health equity is an often-cited goal of public health, included among the 4 overarching goals of the Department of Health and Human Services' Healthy People 2020. Yet it is difficult to find summary assessments of national progress toward this goal.
Objectives: To identify variation in several measures of health equity from 1993 to 2017 in the United States and to test whether there are significant time trends.
Design, setting, and participants: Survey study using 25 years of data, from January 1, 1993, to December 31, 2017, from the Centers for Disease Control and Prevention's Behavioral Risk Factor Surveillance System to assess trends in health equity and health justice by race/ethnicity, sex, and income in 3 categories by year.
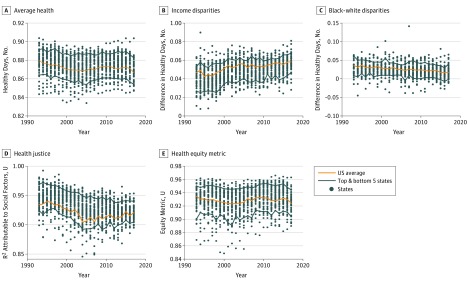
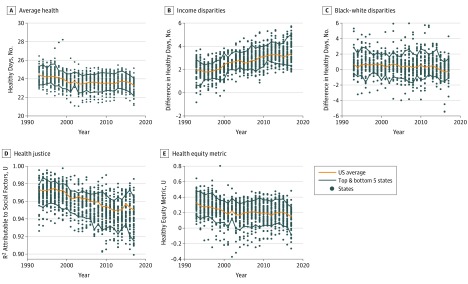
Main outcomes and measures: Health equity was assessed separately for each of 2 health constructs: healthy days-the average of physical and mental healthy days over the previous 30 days-and general health in 5 categories, rescaled to approximate a continuous variable. For each health construct, average health was calculated along with 4 measures of health equity: disparities across 3 income groups; black-white disparities; health justice-a measure of the correlation of health outcomes with income, race/ethnicity and sex; and a summary health equity metric.
Results: Among the 5 456 006 respondents, the mean (SD) age was 44.5 (12.7) years; 3 178 688 (58.3%) were female; 4 163 945 (76.3%) were non-Latinx white; 474 855 (8.7%) were non-Latinx black; 419 542 (7.7%) were Latinx; and 397 664 (7.3%) were of other race/ethnicity. The final sample included 5 456 006 respondents for self-reported health and 5 349 527 respondents for healthy days. During the 25-year period, the black-white gap showed significant improvement (year coefficient: healthy days, 0.021; 97.5% CI, 0.012 to 0.029; P < .001; self-reported health, 0.030; 97.5% CI, 0.025 to 0.035; P < .001). The health equity metric for self-reported health showed no significant trend. For healthy days, the Health Equity Metric declined over time (year coefficient: healthy days, -0.025; 97.5% CI, -0.033 to -0.017; P < .001). Health justice declined over time (year coefficient: healthy days, -0.045; 97.5% CI, -0.053 to -0.038; P < .001; self-reported health, -0.035; 97.5% CI, -0.046 to-0.023; P < .001), and income disparities worsened (year coefficient: healthy days, -0.060; 97.5% CI, -0.076 to -0.044; P < .001; self-reported health, -0.029; 97.5% CI, -0.046 to -0.012; P < .001).
Conclusions and relevance: Results of this analysis suggest that there has been a clear lack of progress on health equity during the past 25 years in the United States. Achieving widely shared goals of improving health equity will require greater effort from public health policy makers, along with their partners in medicine and the sectors that contribute to the social determinants of health.
Conflict of interest statement
Figures
References
-
- Murray CJ, Salomon JA, Mathers CD, Lopez AD; World Health Organization. Summary Measures of Population Health: Concepts, Ethics, Measurement and Applications. Geneva, Switzerland: World Health Organization; 2002.
-
- Frank LD, Sallis JF, Conway TL, Chapman JE, Saelens BE, Bachman W. Many pathways from land use to health: associations between neighborhood walkability and active transportation, body mass index, and air quality. J Am Plann Assoc. 2006;72(1):75-87. doi:10.1080/01944360608976725 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
