

Association of Titin-Truncating Genetic Variants With Life-threatening Cardiac Arrhythmias in Patients With Dilated Cardiomyopathy and Implanted Defibrillators
- PMID: 31251381
- PMCID: PMC6604081
- DOI: 10.1001/jamanetworkopen.2019.6520
Association of Titin-Truncating Genetic Variants With Life-threatening Cardiac Arrhythmias in Patients With Dilated Cardiomyopathy and Implanted Defibrillators
Abstract
Importance: There is a need for better arrhythmic risk stratification in nonischemic dilated cardiomyopathy (DCM). Titin-truncating variants (TTNtvs) in the TTN gene are the most common genetic cause of DCM and may be associated with higher risk of arrhythmias in patients with DCM.
Objective: To determine if TTNtv status is associated with the development of life-threatening ventricular arrhythmia and new persistent atrial fibrillation in patients with DCM and implanted cardioverter defibrillator (ICD) or cardiac resynchronization therapy defibrillator (CRT-D) devices.
Design, setting, and participants: This retrospective, multicenter cohort study recruited 148 patients with or without TTNtvs who had nonischemic DCM and ICD or CRT-D devices from secondary and tertiary cardiology clinics in the United Kingdom from February 1, 2011, to June 30, 2016, with a median (interquartile range) follow-up of 4.2 (2.1-6.5) years. Exclusion criteria were ischemic cardiomyopathy, primary valve disease, congenital heart disease, or a known or likely pathogenic variant in the lamin A/C gene. Analyses were performed February 1, 2017, to May 31, 2017.
Main outcome and measures: The primary outcome was time to first device-treated ventricular tachycardia of more than 200 beats/min or first device-treated ventricular fibrillation. Secondary outcome measures included time to first development of persistent atrial fibrillation.
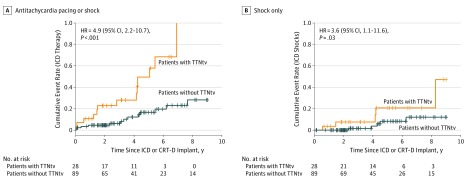
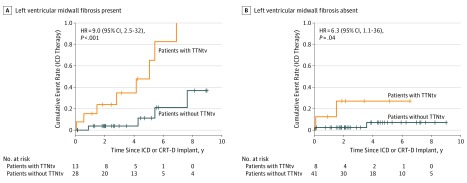
Results: Of 148 patients recruited, 117 adult patients with nonischemic DCM and an ICD or CRT-D device (mean [SD] age, 56.9 [12.5] years; 76 [65.0%] men; 106 patients [90.6%] with primary prevention indications) were included. Having a TTNtv was associated with a higher risk of receiving appropriate ICD therapy (shock or antitachycardia pacing) for ventricular tachycardia or fibrillation (hazard ratio [HR], 4.9; 95% CI, 2.2-10.7; P < .001). This association was independent of all covariates, including midwall fibrosis measured by late gadolinium enhancement on cardiac magnetic resonance images (adjusted HR, 8.3; 95% CI, 1.8-37.6; P = .006). Having a TTNtv was also associated with the risk of receiving a shock (HR, 3.6; 95% CI, 1.1-11.6; P = .03). Individuals with a TTNtv and fibrosis had a greater rate of receiving appropriate device therapy than those with neither (HR, 16.6; 95% CI, 3.5-79.3; P < .001). Having a TTNtv was also a risk factor for developing new persistent atrial fibrillation (HR, 3.9; 95% CI, 1.3-12.0; P = .01).
Conclusions and relevance: Having a TTNtv was an important risk factor for clinically significant arrhythmia in patients with DCM and ICD or CRT-D devices. Having a TTNtv, especially in combination with midwall fibrosis confirmed with cardiovascular magnetic resonance imaging, may provide a risk stratification approach for evaluating the need for ICD therapy in patients with DCM. This hypothesis should be tested in larger studies.
Conflict of interest statement
Figures
References
-
- Shun-Shin MJ, Zheng SL, Cole GD, Howard JP, Whinnett ZI, Francis DP. Implantable cardioverter defibrillators for primary prevention of death in left ventricular dysfunction with and without ischaemic heart disease: a meta-analysis of 8567 patients in the 11 trials. Eur Heart J. 2017;38(22):1738-. doi:10.1093/eurheartj/ehx028 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
